Pituitary tumour apoplexy with visual field defects in pregnancy managed with bromocriptine, hydrocortisone and thyroxine
DECLARATIONS
Competing interests
None declared
Funding
None
Ethical approval
Written informed consent was obtained from the patient or next of kin
Guarantor
RMF Van Der Weiden
Contributorship
NMJ performed the literature search and executed the subsequent and final versions of the manuscript; HD wrote the initial version of the manuscript; RMFVDW supervised treatment of the patient and preparation of the manuscript
Reviewer
Chung Thong Lim
Case report
Neuritis retrobulbaris was diagnosed in a 27-year-old nulligravid woman with an uneventful medical history. The condition spontaneously resolved within 2 months. Magnetic resonance imaging (MRI) was performed and by coincidence a pituitary tumour was found without suprasellar expansion or compression of the optic chiasma of 10 mm. The patient wanted to become pregnant and discontinued oral contraceptive use 2 months earlier. There was no galactorrhoea. Endocrinological analysis revealed a hyperprolactinemia of 3138 μMo1/1. The diagnosis of a microprolactinoma with subsequent hyperprolactinemia suspected of causing secondary amenorrhoea was made. Bromocriptine 2.5 mg medication was started twice daily. Soon thereafter the patient became pregnant and the bromocriptine medication was ceased. At 10 weeks’ of gestation she presented with a continuous headache and visual complaints of the left eye. Endocrinological tests demonstrated an increased prolactin concentration of 5660 μMo1/1 and a disruption of the pituitary-thyroid axis and the pituitary-adrenal axis (Table 1). Visual field examination disclosed defects compatible with compression of the optic chiasm and MRI demonstrated tumour growth of the prolactinoma, suprasellar extension and a marked compression of the optic chiasm. Liquefaction was seen within the prolactinoma, indicating an apoplexy within the tumour, at this moment diagnosed as a macroprolac-tinoma. (Figure 1A)
Summary of endocrine biochemical results
References
Before therapy
At the time of conception
10 weeks
19 weeks
33 weeks
37 weeks
5 weeks post partum
TSH
0.4-4.2 mU/l
3.6
2.8
0.93
0.85
0.059
0.028
0.021
FT-4
11-21 pmol/l
14
16
11
9
12.9
14.5
16.7
Prolactin
60-500 mU/l
3138
95
5660
509
331
273
77
Cortisol
0.18-0.72 μMol/L
0.45
-
-
0.22
0.78
1.02
0.36
ACTH
7-50 ng/l
18
-
-
15
-
-
<5.0
MRI T1 showing liquefaction within the pituitary tumour (a) MRI taken at a gestational age of 10 week. Pituitary tumour of 19,5 mm, evidence of a liquid level, suitable with an apoplexy within the prolactinoma. Strong compression of the optic chiasm with cranial movement. (b) MRI taken 5 weeks postpartum. Pituitary tumour of less than 10 mm, little impression of the sphenoidal sinus. Pituitary stalk is removed to the left.
Both neurosurgical treatment and medication was considered, and the latter was chosen because of the patients’ pregnancy. Medication consisted of bromocriptine 2.5 mg twice daily, levothyroxine 150 μg once a day and hydrocortisone three times a day in the following dose scheme: 15 mg-7.5 mg-7.5 mg. At 19 weeks of pregnancy, the headache disappeared, prolactin levels decreased and visual field defects improved. At 33 weeks of pregnancy, laboratory values and visual field examination were returned to normal. (Table 1) Medication was continued and the further course of pregnancy was uneventful. The patient was delivered vaginally of a healthy daughter of 3300 g at 40 weeks’ of gestation. The mother had no wish to take up breastfeeding. Six weeks after delivery there were no physical complaints and no visual field deficits. MRI showed a major decline of the adenoma. (Figure 1B) Thyroxine could be discontinued at that time, hydrocortisone and bromocriptine were continued.
Discussion
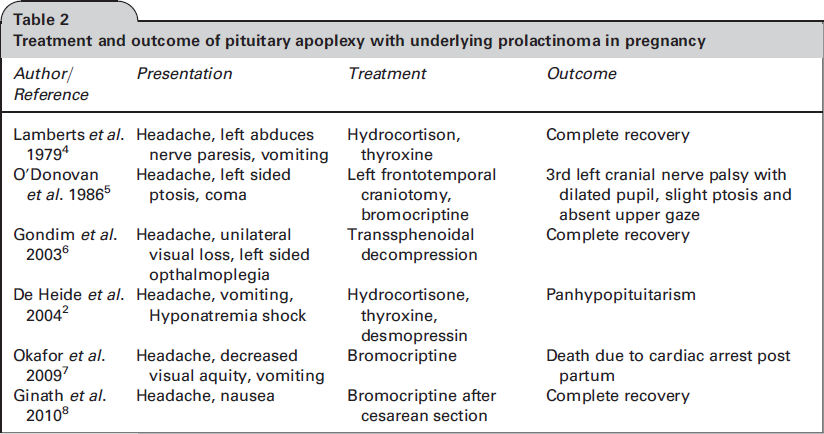
Lactotrophic cells of the anterior pituitary gland are covered with oestrogen receptors mediating hyperplasia of these lactotrophic cells and thus a physiological increase of the prolactin producing part of the pituitary gland during pregnancy.1 The combination of a pituitary adenoma and this physiological increase may compromise the blood supply, either leading to infarction or haemorrhage.2 Pituitary tumour apoplexy refers to a clinical syndrome consisting of a constellation of signs and symptoms that occur with rapid expansion of the contents of the sella turcica. The occurrence during pregnancy is rare and there have been twelve case reports of pituitary apoplexy during pregnancy of which only six evolved from prolactinomas (Table 2). The earliest symptoms of a pituitary apoplexy are sudden and severe, retro-orbital, bifrontal or suboccipital headache, which may be accompanied by nausea and vomiting.2 The increase in intra-sellar pressure can lead to compression and necrosis of pituitary tissue resulting in hypopituitarism. The increased pressure can also endanger cranial nerves in cavernous sinus (cranial nerves III, IV, V, and VI). Clinically, such an extension is seen in 70% of patients, which can cause diplopia and other manifestations of cranial nerve palsies.3
Treatment and outcome of pituitary apoplexy with underlying prolactinoma in pregnancy
MRI and endocrinological evaluation are essential diagnostic tools for diagnosis and follow-up. Initial management in acute pituitary apoplexy consists of replacement of the deficient hormones, especially corticosteroid to treat adrenal insufficiency and the effects of edema on suprasellar structures.2,3 Following stabilization there is no consensus regarding the treatment of pituitary apoplexy in pregnant patients: transsphenoidal resection or medical treatment with dopamine agonists and corticosteroids. The latter is the first choice of treatment in patients without visual field defects and in patients with a rapid improvement of visual field defects.3 Transphenoidal resection was performed in those cases presenting with major symptoms (Table 2). Corticosteroids should be maintained as replacement therapy. No teratogenic side effects have been reported of bromocriptine administration during conception and pregnancy.3 This case report indicates that even in patients with a major pituitary apoplexy and visual field defects in pregnancy, conservative medical treatment should be the first choice of treatment.
Footnotes
Acknowledgments
None
References
1.
CasanuevaFF, MolitchME, SchlechteJA. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas.Clinical Endocrinology2006; 65: 265–273.
2.
De HeideLJM, van TolKM, DoorenbosB. Pituitary apoplexy presenting during pregnancy.Neth J Med2004; 62: 393–6.
3.
NawarRN, AbdelMannanD, SelmanWR, ArafahBM. Pituitary Tumor Apoplexy: A review.J J Intensive Care Med2008; 23: 75–90.
4.
LambertsSW, KlijnJG, de LangeSA, SinghR, StefankoSZ, BirkenhagerJC. The incidence of complications during pregnancy after treatment of hyperprolactinemia with bromocriptine in patients with radiologically evident pituitary tumors.Fertil Steril1979; 31: 614–9.
5.
O'DonovanPA, O'DonovanPJ, RitchieEH, FeelyM, JenkinsDM. Apoplexy into a prolactin secreting macroadenoma during early pregnancy with successful outcome. Case report.Br J Obstet Gynaecol1986; 93: 389–91.
6.
GondimJ, Ramos JúniorF, PinheiroI, SchopsM, Telia JúniorOI. Minimal invasive pituitary surgery in a hemorrhagic necrosis of an adenoma during pregnancy.Minin Invasive Neurosurg2003; 46: 173–6.
7.
OkaforU, OnwuekweI, EzegwuiH. Management of pituitary adenoma with mass effect in pregnancy: a case report.Cases J.2009; 30;2:9117.