
Abstract
The Royal College of Radiologists (RCR) published guidelines in 2003 which aimed to standardise and improve the safety of sedation in the modern Radiology department. As sedation requirements increase, we decided to audit our own departments understandings and practice with respect to sedation. A repeat audit cycle was performed following a re-educational lecture, one year later. Three common sedation case scenarios were incorporated into a questionnaire which detailed questioning on requirements for fasting, monitoring and the order and use of sedation drugs alongside analgesics. These were compared to the 2003 RCR guidelines. The audit was recycled at one year. Despite the RCR guidelines, freely available on the RCR website, there was a persisting variation in practice which revealed a lack of awareness of the requirements for adequate fasting and the importance of giving the opiate before the benzodiazepine (sedative) agent in cases where a combination are chosen. The audit did show a trend towards using shorter acting benzodiazepines, which is in keeping with the guidelines. Monitoring of vital signs was generally, well carried out. General awareness of the RCR guidelines for safe sedation in the Radiology department was initially low and practice found to be variable. Re-education saw some improvements but also, some persisting habitual deviations from the guidelines, particularly with respect to the order in which the opiate and sedative benzodiazepine were given.
Introduction
The Royal College of Radiologists (RCR) published guidelines in 2003 entitled ‘Safe sedation, analgesia and anaesthesia within the Radiology Department’. 1 These were partially based on guidelines issued by the Academy of Medical Royal Colleges in 2001. This was prompted by concerns raised about the safety of sedation techniques used for health care procedures by different specialty groups and that guidance on the safe use of sedative drugs is often not followed, either through lack of awareness, lack of training or insufficient staff due to financial constraints, leading to exposure to unnecessary patient risk. The nature of procedures undertaken in a radiology department leads to an increasing requirement for sedation and analgesia techniques to be practised well. 4
Within the guidelines, certain areas were identified as potential sources of risk. These highlighted fasting status, drug choices and dosing recommendations, specific monitoring requirements and the order of drug administration as the major areas of concern.
After an index case (unexpected respiratory arrest during biliary drainage), we decided to audit our current sedation practice in an attempt to minimize any further potentially avoidable adverse incidents, institute some further education and then re-audit after a year had passed.
Methods
A questionnaire was circulated to all radiology consultants and senior trainees within the department, which targeted several areas of concern with sedation practice. Details on any requirement for patient fasting, the choice of sedative and analgesic drugs and their corresponding initial dose, if used, and specific monitoring details were requested. The questionnaire also asked for details of the order of administration of the analgesic and sedative drugs, if given in combination.
It is recognized that sedation should be tailored to the individual patient and scenario, and to accommodate this, the questionnaire used three common clinical scenarios to gather the data.
The three scenarios were:
A 50-year-old, 70 kg man, requiring tunnelled central venous catheter line access for chemotherapy; A 55-year-old, 70 kg man, requiring percutaneous nephrostomy for obstruction but who was not clearly septic; A frail 80-year-old, 50 kg woman, with Chronic Obstructive Airways Disease (COPD) and ischaemic heart disease, requiring percutaneous transhepatic drainage for obstructive jaundice with sepsis.
The purpose was to audit whether guidelines were adhered to, if sedative or analgesic agents were used. It was not the aim to assess whether these agents were required.
Along with lessons learned from the index case, the results from this survey were followed up in an initial departmental presentation aimed at feedback and education, making clear reference to the recent college guidelines. Consultants, trainees and nurses attended this meeting. Further training was arranged over the subsequent year. A second identical survey was carried out one year later, to assess whether there had been any change.
Results
There were 14 returns from the first survey (2005) and 13 returns from the subsequent survey (2006). Of these, five (2005) and three (2006) said they would use sedation for case 1, while five (2005) and four (2006) would use sedation for case 2, and finally, nine (2005) and seven (2006) would use sedation for case 3.
Fasting requirements before sedation
The initial audit showed variable practice and a lack of appreciation of the need for appropriate fasting before the administration of a sedative. Current guidelines recommend a regimen similar to that required for a patient receiving a general anaesthetic, namely, four hours for solids and ideally two hours for fluids (Figure 1). The subsequent audit showed that all practitioners were now aware of this requirement.
Fasting before sedation
Which sedative agent?
Both audits showed that practitioners used a shorter acting benzodiazepine, midazolam, rather than the less predictable, longer acting diazepam or lorazepam when required (Figure 2). This is in keeping with the recommendations made by the college guidelines.
Sedative choice
Which analgesic agent?
Between the two audits, there has been a move to the use of fentanyl, particularly from pethidine and morphine (Figure 3). Diamorphine has become the only alternative agent used. The feeling of senior anaesthetic colleagues is that practitioners use the drug that they and their staff are most familiar with.
Analgesic choice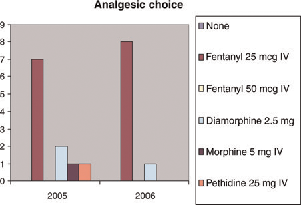
Sedative or analgesic first?
Guidelines advise giving the opiate before benzodiazepine, if both agents are required. This may not always be possible as additional analgesia may be required during the procedure. However, it is important to recognize that the risk of significant respiratory depression is increased if the agents are given in the reverse order. This was not recognized by practitioners in our department in the initial audit, and despite marked emphasis being placed upon this during the education process (it was a major factor in the index case), there was no change in the second audit with just under half of the practitioners persisting in giving the benzodiazepine first drug first (Figure 4).
Which drug first?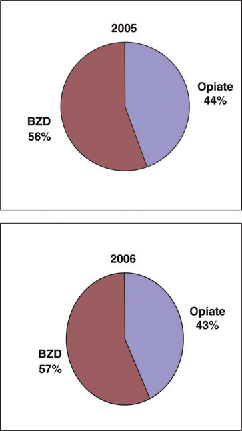
Monitoring
The responses to both questionnaires showed that practitioners had a good appreciation of the need for careful cardiorespiratory monitoring and that this task is best delegated to a trained member of the staff, who is not directly involved in the practical aspects of the actual procedure itself. In our department, nurses trained in the administration of sedation and analgesia attend all relevant procedures whether in hours or on-call.
Discussion
The initial survey carried out within the department, highlighted the areas of sedation practice that required review and education, with the most notable perhaps, being the need for appropriate fasting both for solids and fluids. The re-audit showed that the educational process was effective in addressing this. During the year, the number of different opiate analgesic drugs used locally, decreased from four to two. Midazolam was used in all cases when additional sedation was required.
However, a persistent deficit in our current practice was the lack of knowledge of the importance of giving opiate analgesia before additional sedation, if this is required, with almost half our sample group routinely giving these agents in the reverse order. This has been a focus of our educational process directed to practitioners and also attending nurses, so that reminders can be given.
When necessary, incremental observed analgesia and sedation is the safest way to manage patients who do not require a general anaesthetic in the radiology department. This cannot be done adequately by the operator, and attendance of appropriately trained nursing staff is essential.
Knowledge of the patient's medical background and current condition allied with proper fasting, individual monitoring and rational use of appropriate drugs in a structured manner, should help to make the increasing demands for sedation in the modern radiology department as safe as possible. It is important to use index cases as an opportunity and focus for continuing education.