
Abstract
Laparoscopic fundoplication is an established treatment for refractory gastro-oesophageal reflux disease. This study aims to compare the outcome of two laparoscopic antireflux techniques in a regional specialist unit. A sequential audit was carried out on patients undergoing laparoscopic Nissen (LN: performed May 1994 to November 2000) or laparoscopic anterior (LA: performed March 2001 to December 2004) fundoplication. Patient satisfaction was assessed by postal questionnaire. The cohorts undergoing each operation were also divided into two chronological groups of 51 patients, to study the effect of possible learning curve progression on the number of nights spent in the hospital postoperatively. In all, 142/204 (70%) questionnaires were returned from patients with follow-up ranging from 5 to 40 months postoperation. Overall, 102/142 (72%) reported a good or excellent outcome. Patients who underwent LA had a higher rate of antacid medication use (LN 17.4% versus LA 34.2%, P = 0.036) but there was a higher score for inability to belch following LN (LN 2.03 versus LA 1.53, P = 0.034). When comparing the chronologically divided cohorts, LN was associated with a significantly longer hospital stay than LA (P < 0.001, Mann-Whitney U test). There was a significant decrease in hospital stay from the first to second group of 51 LNs (P < 0.001, Mann-Whitney U test) and a further significant reduction in hospital stay from the first 51 to second 51 LAs (P < 0.001, Mann-Whitney U test). In conclusion, both procedures provide good symptom control. Increased requirement for acid suppression following LA and inability to belch following LN, may suggest more long-term durability of the LN wrap. The decrease in the number of nights spent in hospital may be related to the procedure performed but seems more likely to be an effect of increasing volume of surgical experience.
Introduction
Gastro-oesophageal reflux disease (GORD) is common, affecting approximately 10–20% of the Western population. 1 Antireflux surgery aims to permanently cure GORD, and is indicated in patients whose symptoms are poorly controlled by acid suppressive drugs, who are intolerant of the side-effects or who do not wish to take long-term medication. 2
The most frequently performed operation is the Nissen fundoplication, producing a 360° wrap of fundus around the lower oesophagus. Nissen fundoplication is highly successful at controlling symptoms, with greater than 90% patient satisfaction in 12 months.3,4 Recently, numbers of operations performed for refractory GORD have increased, possibly reflecting the widespread adoption of the laparoscopic approach.2,2 A randomized controlled trial (RCT) showed laparoscopic Nissen (LN) fundoplication to be associated with reduced postoperative pain, analgesic requirements and time to solid food intake when compared with the open procedure. 6 Some concerns were initially raised when a study group in the Netherlands were forced to abandon a large RCT comparing laparoscopic with open Nissen fundoplication, due to an excess incidence of dysphagia in the laparoscopic procedure. 7 Reassuringly, a more recent study of laparoscopic and open Nissen procedures performed in the UK, showed similar levels of postoperative dysphagia following both operations. 8
The laparoscopic anterior fundoplication (180° wrap) aims to reduce the incidence of common adverse effects such as dysphagia, bloating and inability to belch (the ‘gas-bloat’ syndrome) and has good results.8,9 Although physiological studies have shown that both procedures increase lower oesophageal sphincter pressure, as measured by manometry, the Nissen fundoplication produces significantly higher gastric pressure upon stomach distension and may be responsible for increased ‘gas-bloat’. 10
A major attraction of laparoscopic fundoplication is that it can be performed as a day-case procedure. In a study of 20 patients undergoing LN, performed to assess the acceptability and safety of same-day discharge, everyone was discharged the same day and 19/20 patients stated that they would undergo the same procedure again as a day-case. 11 In the UK, rapid growth of day surgery and dedicated day-case units over the last 10–20 years has dominated surgical practice. 12 Reduction in acute hospital beds has led to increased government pressure to maximize therapies provided within a predictable timeframe. Both LN and laparoscopic anterior (LA) are acceptable for same-day discharge, but no group has studied differences between the operations in this respect.
Our department changed the standard antireflux operation performed from LN to LA in 2001, for a variety of reasons, but foremost because of increasing evidence that LA seemed to be associated with lower postoperative problems. The aim of this study was to evaluate the effect of this change on the reported longer-term symptoms and length of postoperative hospital stay.
Patients and methods
Patients
All consecutive patients undergoing primary laparoscopic antireflux surgery in a single specialist upper gastrointestinal unit between May 1994 and December 2004, were identified using the Lothian Surgical Audit (LSA) database, with validation by retrospective case-note review. All procedures were performed or assisted by two consultant upper gastrointestinal surgeons. Patients requiring management of an intrathoracic stomach or undergoing revisional surgery were excluded. Decision for discharge was made by the surgeon after reviewing the patient postoperatively.
Two different procedures were studied: LN fundoplication (operations performed from May 1994 to November 2000) and LA fundoplication (operations performed from March 2001 to December 2004). The cohorts undergoing each operation were then divided into two chronological groups of 51 patients each, giving a total of four groups (2 groups of LNs and 2 groups of LAs). These clusters were used to represent the early (first 51 procedures) and later (second 51 procedures) experiences of both LN and LA.
Technique
LN and LA fundoplication are described elsewhere.13,14 Briefly, both involved reduction of any hiatus hernia and mobilization of the fundus of the stomach by division of the short gastric vessels for LN. Crural repair was performed routinely behind the oesophagus for both procedures. For LN, a 360° posterior fundoplication was carried out over a 54F bougie for a length of approximately 3 cm. For LA, the anterior part of the gastric fundus was sutured over the anterior surface of the lower oesophagus as a 180° fundoplication.
Questionnaire
Patients were sent postal questionnaires at a single time-point for each cohort (mean 22 months follow-up), analysed anonymously. The questionnaire included a DeMeester score to evaluate symptoms of GORD (heart-burn, acid regurgitation and dysphagia). Each question was scored from 0 = none to 3 = everyday. Total scores ranged from 0 to 9 (maximum symptoms). 14 An additional question on the same scale (0–3) was included regarding painful bloating, and the sum of all four questions was taken as the modified DeMeester score (range 0–12).
The Gastrointestinal Symptom Rating Scale (GSRS) is a validated series of 15 questions, which is used to produce five subscales with mean scores for reflux, diarrhoea, constipation, abdominal pain and indigestion. 15 Higher scores denote the highest level of symptoms. Two additional questions on the same scale (1–7) were included regarding the inability to vomit and belch.
Patients were also asked to rate the success of their operation and list all current medications.
Statistical analysis
Differences between groups were considered significant at P < 0.05. No adjustment was made for multiple testing.
The difference in male/female ratios was compared using the chi-square test with continuity correction. Mean age between the two operative groups was compared using the two-sample t-test. Length of hospital stay was analysed using the Mann-Whitney U test. The difference in the length of hospital stay between the four chronological patient groups (early LN, late LN, early LA and late LA) was compared using the Kruskal–Wallis test. Hospital stay was then categorized into four groups: 0, 1, 2 and 3 or more nights spent in hospital, for the ease of graphical representation.
Calculations were performed using SPSS (version 14; SPSS Inc., Chicago, IL, USA).
Results
Patient demographics and questionnaire response
There was no difference between the operative groups in terms of age or gender (Table 1). Two patients in the LN group had a wound infection, one LA and two LN patients had urinary tract infections, and five LA and six LN patients had chest infections during their recovery. There were two cases of dysphagia requiring intervention in the LA group and one pleural effusion secondary to a pleural breach in the LN group.
Demographics of each operative group
Questionnaires were sent to 185/204 patients with up-to-date contact information. Of these, 69/83 LN (83%) and 73/102 LA (72%) responses were received.
Level of symptoms present at follow-up
Table 2 shows the mean symptom scores. Overall, symptom control was good with 85.2% of patients reporting none, or only occasional episodes of heart-burn. There was no significant difference between LN and LA in the reflux scores assessed by the questionnaire. However, there appeared to be a trend towards lower values in the LN group. The distribution of the DeMeester symptom score in both groups is illustrated in Figure 1.
Distribution of DeMeester scores (Mann-Whitney U test, P = 0.098). LN, laparoscopic Nissen; LA, laparoscopic anterior
Comparison of questionnaire-derived mean symptom scores

GSRS, Gastrointestinal Symptom Rating Scale
There was significantly more inability to belch in patients who had undergone LN (Table 2), but no significant difference in gas bloat (LN 2.00 versus LA 1.71, Mann-Whitney U test, P = 0.513).
Relationship between time at follow-up and symptoms
There was no correlation between length of time since surgery and either modified DeMeester score or GSRS reflux score.
Patients with LN fundoplication showed a significant improvement in symptoms of gas bloat (Spearman's rank, r = -0.254, P = 0.017) and inability to belch (Spearman's rank, r = -0.273, P = 0.012) with increasing time since operation. There was no such correlation in the LA group.
Success of operation
In all, 102/142 patients (71.8%) reported a good or excellent result. Only 14 (9.9%) reported a poor result. Reported success of surgery correlated significantly with low levels of all assessed symptoms, and most strongly with a low modified DeMeester score (Spearman's rank, r = -0.696, P < 0.001) and GSRS reflux (Spearman's rank, r = -0.651, P < 0.001) scores. There was no difference in the distribution of perceived success of the operation between LN and LA (Figure 2).
Perceived success of operation (χ2 test, P = 0.972). LN, laparoscopic Nissen; LA, laparoscopic anterior
Additional medication
Thirty-seven patients (26.1%) required additional acid-suppression therapy following surgery. There was significantly more regular acid-suppressive medication usage after LA (LN 17.4% versus LA 34.2%, Yate's χ2 test, P = 0.036) (Figure 3).
Use of acid-suppression medication following surgery (Yate's corrected χ2 test, P = 0.036). LN, laparoscopic Nissen; LA, laparoscopic anterior
Patients using additional medication had significantly higher scores for all parameters of acid reflux. Those using medication regularly had a mean DeMeester score of 2.92 when compared with 1.27 for non-medicated patients (Mann-Whitney U test, P < 0.001). This indicates that the reported use of additional antacid medication correlates well with increased symptoms of reflux: 7.7% of patients with a DeMeester score 0 used additional acid suppression, 13.3% with score 1, 37.5% with score 2 and 55.6% with score 3 or more. There was also an associated deterioration in the perceived success of surgery in patients requiring antireflux medication (Mann–Whitney U test, P < 0.001): 81% of patients who did not require additional medical therapy, reported a good or excellent outcome, when compared with corresponding reports from only 46% of those who required some form of treatment.
Length of stay in the hospital
Overall, 19 people were discharged on the day of operation, 94 stayed one night, 65 stayed two nights and 26 remained in the hospital for three nights or more (Table 3). The rate of discharge within 23 hours (one night or less) was 113/204 (55.4%).
Patients staying for the illustrated length of time for sequential operative groups (n)

There was a significant difference between LN and LA in terms of the length of time until discharge (P < 0.001, Mann–Whitney U test) (Figure 4). LA patients spent a median of one night (range 0–6) in the hospital, while those undergoing LN required a median of two nights (range 0–26).
Comparison of the overall length of stay in the hospital for each operative group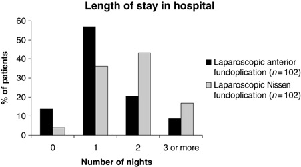
Discussion
This study has shown that both LN and LA fundoplication provide a high level of patient satisfaction, although there is a slight tendency towards the use of more acid-suppressive medication in the LA group, perhaps suggesting that LA is less effective in the longer term. Despite this, there is no difference between the groups in reported recurrence of symptoms. These results are in agreement with previous RCTs that have shown no difference between the operations in mean heart-burn scores.9,11 There was also an overall reduction in hospital stay as the quantitative experience of the unit increased and a shorter stay in hospital after LA compared with LN.
Our findings revealed significantly more inability to belch in the LN cohort but this was not accompanied by other ‘gas-bloat’ symptoms or dysphagia. Nonetheless, a significant negative correlation between time since operation and both inability to belch and a sensation of bloatedness, was only present in the LN group. This may indicate that LN causes ‘gas-bloat’ syndrome in the early postoperative period but this subsequently improves with time, which is in concordance with other studies that indicate patients are more likely to be able to belch following LA.9,16 However, manometry performed after fundoplication has shown that the altered oesophageal sphincter anatomy means that patient-reporting of this symptom is unreliable. 17
Patients undergoing LA had a higher rate of use of acid-suppressive medication, a result that has been noted previously when comparing LA, LN and open Nissen fundoplications. 8 The fact that medication usage was associated with a higher DeMeester score, and thus worse GORD symptoms, suggests that mean reflux scores for the LA group were at best only marginally lowered by antacids. Most patients using acid suppression following fundoplication, do not have abnormal oesophageal acid exposure. 18 Nevertheless, these results might suggest a greater requirement to suppress residual reflux disease in patients who have had LA instead of LN fundoplication and therefore a higher risk of ‘loosening of the wrap’ in these patients.
The group from Adelaide, Australia demonstrated no difference between the LN and LA groups in terms of the commencement of oral fluids (median 1 day), solids (median 2 days) and the length of postoperative stay (median 3 days) in their first RCT. 9 Another trial published six years later from South Africa also showed no difference in time of discharge between LN and LA. 19 Interestingly, patients in this trial started oral fluids immediately and had a median stay of two days; one day faster than Adelaide. However, these studies were not specifically conducted to investigate the length of stay and therefore were not analysed in terms of accumulating operative experience.
Only one previous study evaluated postoperative stay following open with LN fundoplication. Postoperative stay was significantly shorter in the laparoscopic group, although both groups stayed a median of three days in hospital. 20
Hwang et al. 21 looked at the learning curve for the first 100 laparoscopic fundoplications. Similar to our study, these procedures were performed by two surgeons and the first 50 cases were used to represent the early institutional experience. They demonstrated a significant decrease in operative time with increasing experience, but no change in the mean length of postoperative stay (2.5 days). None of these studies have managed to achieve our median rate of discharge for LA patients of one night. The largest analysis performed to date, studied 24,208 antireflux surgical procedures between 1990 and 1997 in US hospitals and demonstrated a decrease in the median length of hospital stay from seven to two days. However, this study included open abdominal, thoracic and laparoscopic procedures, and there was an increase in the proportion of operations performed laparoscopically from 0.5% in 1990, to 64% in 1997. 22
In conclusion, both LA and LN operations provide a high level of patient satisfaction. The higher incidence of inability to belch following LN, appears to decrease with time and may represent recovery from symptoms of the ‘gas-bloat’ syndrome. The higher rate of acid-suppression medication following LA, may suggest that it is less ‘durable’ than LN, although there is no objective evidence of significantly increased recurrence of acid reflux. The possible, better, long-term control of reflux associated with a 360° wrap, is counterbalanced by a slightly greater risk of complications due to increased gastric pressure upon distension.
Finally, the ability seen in our study to discharge patients on the day of operation or after one night in the hospital, is likely to be related to both the change in operation type from LN to LA and the accumulating experience of the department. Analysis of the total operative time and the multifactorial nature of the discharge decision might have been useful but were not recorded. Any benefit is most likely to be found in cost-savings in terms of time spent in the hospital, as the clinical benefit would probably be negated by an increased convalescence time at home.
Footnotes
Acknowledgement
This paper was previously presented as an abstract at the Association of Surgeons of Great Britain and Ireland conference in Edinburgh in 2006.