
Abstract
Prescribing in the perinatal period is based on a risk-benefit analysis, in the context of a limited evidence base, composed primarily of case series and reports. Mothers with depressive illness often present first in the community and effective treatment is paramount for the well being of both mother and child. We aimed at investigating current prescribing practices among general practitioners (GPs) of antidepressants to mothers presenting in first trimester of pregnancy and during breastfeeding. This qualitative study was conducted by way of postal survey to 78 GPs within South Central Edinburgh catchment area. All responses were anonymous and confidential. We discovered inconsistent prescribing patterns among GPs to both pregnant and breastfeeding mothers. Only one GP suggested consulting clinical guidelines when making prescribing choices. There was no mention of the continuation of an antidepressant from pregnancy into breastfeeding as a reason of choice. Inconsistent prescribing patterns among GPs could have implications for the well being of mother and child, and may be reflective of an underlying educational need among GPs.
Introduction
Depressive illness within the perinatal period is common, affecting approximately 10–15% of women1,2 and the consequences of a major depressive episode during this time can be significant. Mothers suffering from untreated depression may experience a variety of difficulties which could include an increased risk in obstetric complications, neglected self-care, substance misuse and an elevated risk of suicide.3–6 The detrimental effects on the infant are also evident, with some studies suggesting that untreated mental disorder within the perinatal period can result in neuropsychological deficit in the affected child. 7 The effective and prompt treatment of depressive illness affecting mothers is therefore of paramount importance.
Over 90% of mothers with depression will be treated in the community, usually by their general practitioner (GP). 8 This prescribing decision should be based on a risk–benefit analysis of the clinical situation, taking into account the relevant evidence base. However, the risk profile for antidepressant use in pregnancy and breastfeeding is based on limited evidence, predominantly composed of case reports and case series, thus making safe prescribing choices a challenge for practitioners.
Methods
Our study was conducted in January 2007, one month prior to publication of National Institute for Heath and Clinical Excellence (NICE) guidelines ‘Antenatal and Postnatal Mental Health’. 9 We mailed surveys to 78 GPs within South Edinburgh catchment area. We asked them to consider two case vignettes:
Case vignette one
A lady presents to you with her first ever episode of depression. She is in her first trimester of pregnancy. The depression is severe enough for you to consider antidepressant treatment. There is no other relevant medical history.
Case vignette two
A lady presents to you with her first ever episode of depression. She is six weeks postpartum and is breastfeeding. The depression is severe enough for you to consider antidepressant treatment. There is no other relevant medical history.
For each vignette, the doctor was required to answer the following questions:
Which antidepressant(s) would you consider as your first choice? Why would you make this choice? Which antidepressant(s) would you avoid? Why would you avoid these medications?
All responses were anonymous and confidential. Data were collected and analysed in Microsoft Excel. Ethical approval was not required.
Results
The overall response rate was 41% (n = 32/78). All clinicians were GPs based with South Central Edinburgh catchment area.
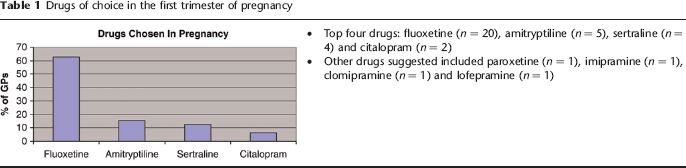
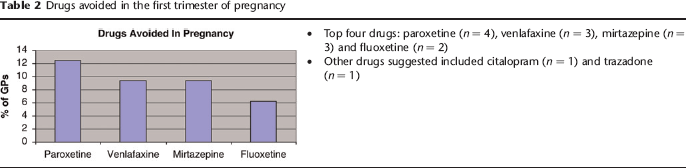
The drugs of choice in first trimester of pregnancy are outlined in Table 1 and those of avoidance in Table 2. There was no restriction on the number of medications which could be selected for this case vignette by each clinician.
Drugs of choice in the first trimester of pregnancy
Drugs avoided in the first trimester of pregnancy
One in four GPs (n = 8) recommended a class of antidepressants rather than a specific drug. These included tricyclic antidepressant (TCAs) (n = 4), selective serotonin reuptake inhibitor (SSRIs) (n = 3) and monoamine oxidase inhibitor (MAOIs) (n = 1). One in 10 GPs (n = 3) preferred not to prescribe an antidepressant at all.
In all, 84.4% GPs (n = 27) recommended avoiding a class of antidepressants rather than a specific drug. These included TCAs (n = 12), MAOIs (n = 9), SSRIs (n = 4) and ‘new drugs’ (n = 2). One in four GPs (n = 8) would avoid ‘all drugs’.
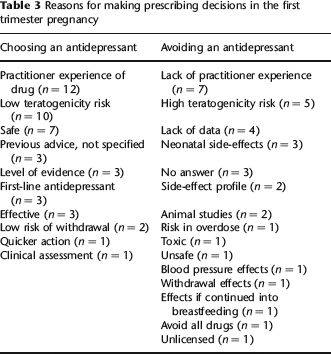
The most common reasons for choosing or avoiding an antidepressant in pregnancy are listed in Table 3.
Reasons for making prescribing decisions in the first trimester pregnancy
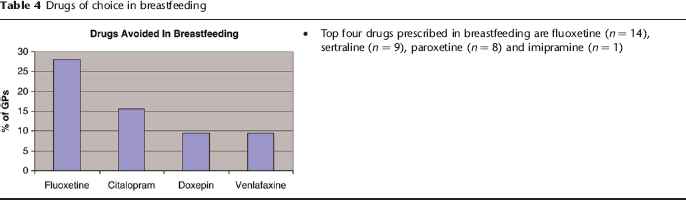
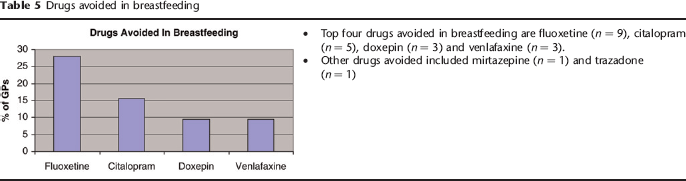
The drugs of choice in breastfeeding are outlined in Table 4 and those of avoidance in Table 5. Again, there was no restriction in the number of medications which clinicians were allowed to select in this case vignette.
Drugs of choice in breastfeeding
Drugs avoided in breastfeeding
One in four GPs (n = 8) prescribed a class of antidepressant rather than a specific drug. This included TCAs (n = 6) and SSRIs (n = 2). One GP recommended counselling or postnatal support groups. One GP preferred not to prescribe at all.
In all, 68.8% GPs (n = 22) recommending avoiding a class of antidepressant rather than a specific drug. This included TCAs (n = 14), MAOIs (n = 5), ‘newer drugs’ (n = 2) and SSRIs (n = 1). Seven GPs stated they would not prescribe any drugs.
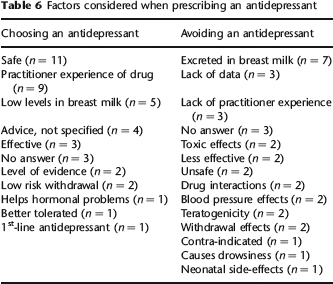
The most common reasons for choosing or avoiding an antidepressant in breastfeeding are listed in Table 6.
Factors considered when prescribing an antidepressant
The sources consulted when making prescribing decisions in both pregnancy and breastfeeding are listed in Table 7.
List of sources consulted in pregnancy and breastfeeding
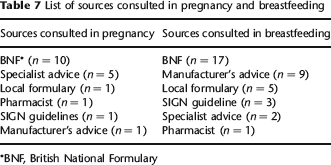
BNF, British National Formulary
Discussion
We have reviewed the GPs recommendations for medications in both scenarios and compared with our gold standard of NICE guidelines ‘Antenatal and Postnatal Mental Health’ (February 2007). 9 It is important to note that these guidelines were not available at the time of our survey.
Overall, it seemed that prescribing patterns among GPs were inconsistent, an example being fluoxetine being both the most favoured and most avoided medication in breastfeeding. It could be speculated that these inconsistencies are related to a lack of practitioner experience or a confusion of reference sources. It was striking that only one GP suggested consulting a set of prescribing guidelines (SIGN) 10 and it may be that this situation has changed since the publication of NICE guidelines in February 2007.
Regarding medications chosen, the majority of medications suggested were in accordance with NICE guidelines as having lower risks within pregnancy and breastfeeding. However, there were several features within the prescribing patterns that give cause for concern. Firstly, there seemed to be a degree of uncertainty when it came to prescribing individual drugs, with a high proportion of GPs stating they would choose an antidepressant from a specific class instead. As there are several medications within each class, with their own individual risk profiles in the perinatal period, this may highlight an area of unsafe prescribing. Secondly, this uncertainty was compounded by several GPs describing a reluctance to prescribe any medications to mothers. While this is understandable from a risk–benefit perspective, the potential for significant consequences for mother and infant resulting from an untreated depressive illness are immense. Thirdly, it is worth noting that there were a number of high-risk medications, for example paroxetine in first trimester (associated with congenital malformations), which were suggested by GPs. Finally it was notable that no GP mentioned the issue of commencing a medication in pregnancy with a view to its continuation into the postpartum period, when a mother wishes to breastfeed. Bearing in mind that most depressive episodes require an average of six months initial treatment and often benefit from a further six months of pharmacotherapy to maintain remission, this point has significant relevance to this group of patients.
Limitations
There are some notable limitations in this study. The absolute number of respondents is low (n = 32) which makes it essential to present these findings in qualitative form. Statistical analysis would be difficult in light of small numbers. The low response rate of 41% also raises the question as to whether there is an element of response bias with those GPs who already feel confident in prescribing or those who take an interest in perinatal psychiatry being the ones to respond.
Despite these limitations, this study provides a snapshot of the prescribing patterns and uncertainties which may be encountered in general practice prescribing. As this study was completed prior to the publication of the relevant NICE guidelines, 9 it would be of value to investigate the impact that these guidelines have had upon GP prescribing. With the ever-evolving evidence base in this area, we feel it is important to address this issue by educating GPs with respect to available prescribing guidelines and to strengthen the links between general adult psychiatry and GPs with a view to providing the best patient-care.