
Abstract
Guidelines suggest that all children with Down's syndrome have hearing testing on a regular basis. Since 2004, the ear, nose and throat (ENT), audiology and education services have conducted a joint clinic for annual ENT health and hearing surveillance of all preschool children with Down's syndrome in Greater Glasgow. The aim of this study is to report the prevalence of ENT problems in this well-defined birth cohort, and the proportion of children for whom ENT surgery is required. A prospective database has been kept since 2004, detailing the ENT health status of every child attending the community-based surveillance clinic. Between September 2004 and September 2008, 87 preschool (aged 9 months to 6 years) children with Down's syndrome were sent appointments for the clinic. Of these, 48 (55%) were female and 39 were male. Data were available for 79 (91%). Over the course of the study, 37% were listed for surgery at some point, either adenotonsillectomy for obstructive symptoms or grommet insertion for otitis media with effusion (OME). The prevalence of OME was 93% at age 1, falling to 68% by age 5. None had significant sensorineural hearing impairment. Obstructive symptoms were also common, with 79% of children having either currently symptomatic upper airways obstruction or a history of adenotonsillectomy by age 5. One child had laryngomalacia and two had symptomatic congenital subglottic stenosis. The prevalence of ENT problems in these children is high. Surgical intervention is frequently required. We advocate a proactive approach of regular ENT and audiology surveillance leading to early intervention, with the aim of maximizing health and educational achievement in the long term.
Keywords
Introduction
Down's syndrome is the commonest chromosomal disorder in humans, and these children are predisposed to a number of problems affecting the ear, nose and throat (ENT). It is unfortunately common for both parents and professionals to have low expectations of children with Down's syndrome, so these problems are often ignored or accepted when they could be treated simply and effectively with improvements in general health and educational achievement.
It is well-known that children with Down's syndrome have a significantly higher incidence of hearing loss than typically developing children. In many cases, however, the studies have been done in a cross-sectional fashion on a population with a large age range. This is not ideal, since the prevalence of hearing problems varies with age. It has been our experience that sensorineural hearing impairment is often progressive and that it tends to affect children of school age. Otitis media with effusion (‘glue ear’, OME), on the other hand, is a problem of preschool children and the prevalence falls as children get older. In addition, these studies are often carried out on children who have been referred to a hospital for treatment,1–4 making it impossible to draw conclusions about how common these problems are in the community. One community-based study from Australia, showed parental report of ear or hearing problems in 57% of children with Down's syndrome aged 5–17 years. 5
Because hearing impairment is so prevalent, the Down's Syndrome Medical Interest Group produced guidelines in 2000 for the hearing surveillance of children and adults with Down's syndrome in the UK, endorsed by various specialty associations and recently revised. 6 It is suggested that all children with Down's syndrome have hearing testing at birth, then at least once a year until they start school, and once every two years thereafter into adulthood.
Hearing impairment is not the only ENT problem to impact upon both education and general health. Obstructive symptoms are common in children with Down's syndrome. Contributing factors include skeletal abnormalities, the large tongue, poor oropharyngeal muscle tone 8 and lingual tonsil hypertrophy.8,9 Chronic sleep disturbance may result with effects on behaviour, concentration and learning. Dyken et al. 10 found Polysomnographic evidence of obstructive sleep apnoea in 15 out of 19 (79%) unselected children with Down's syndrome aged 3–18 years, but so far the only study to look at obstructive symptoms at different ages has been that of Stebbens et al. 11 , who reported symptoms of upper airway obstruction in 9% under one year, 36% between one and two years of age, and 20% between three and four years of age.
The audiology and education services in Greater Glasgow have conducted a joint clinic for annual hearing surveillance of preschool children with Down's syndrome for some time. Since 2004, an ENT surgeon has also been present. This has allowed the detection of obstructive symptoms and other ENT problems at the same time as hearing checks. Regular surveillance allows the identification of potentially remediable problems for which parents may not have sought referral to a hospital clinic. Hospital-based experience of children with Down's syndrome, will underestimate the prevalence of ENT disorders in children with Down's syndrome. Since all children with Down's syndrome in our area are seen at this community-based surveillance clinic, it provides a unique opportunity to report on the ENT health of a well-defined birth cohort followed up over time. The aim of this study is to estimate the prevalence of ENT problems in these children, and the proportion of children for whom ENT input is required.
Subjects and methods
Children with Down's syndrome in Glasgow are referred to our community-based hearing surveillance clinic by a number of different routes. Firstly, at the time of their universal newborn hearing screening test, children identified as being ‘at risk’ of hearing difficulties are referred on for hearing surveillance, and for children with Down's syndrome the referral is to our clinic. All children with developmental delay are under the care of a community paediatrician, who coordinates all aspects of their care, including ensuring that they have regular hearing surveillance. Again, the community doctors refer children with Down's syndrome, to our clinic. This ensures that we are informed of children with Down's syndrome even if they have moved into our area but were born elsewhere. Finally, referrals to the otolaryngology service are redirected to this clinic when the child has Down's syndrome because of the author's interest in this area. By these means, we believe that we have assembled a complete birth cohort for our well-defined geographical area, giving us a unique opportunity to study prevalence.
Every child with Down's syndrome in our area is listed in our database and invited to attend the clinic on an annual basis (or more frequently if there are active problems requiring monitoring). Because they are mostly referred after hearing screening at birth, we see them first at around 9–12 months of age, and continue seeing them until they start school (usually 5 or 6 years of age). Thereafter, the audiometrician sees them at least once every two years in school for hearing surveillance.
At each clinic visit, a structured history and examination are performed, together with age-appropriate hearing testing. The history is taken from the parent or guardian of the child. Audiometric testing is performed by two experienced paediatric audiologists and is tailored to the child's level of ability. In most cases the test used is visual reinforcement audiometry with soundfield presentation, but freefield distraction (Figure 1) and cooperative testing, either soundfield or with headphones (Figure 2), are sometimes used depending on the age and cognitive abilities of the child. It has been rare in our experience for children to be able to tolerate any kind of masking, but bone conduction has occasionally been possible. Tympanometry is used whenever indicated.
Child aged 10 months undergoing freefield distraction hearing testing Same child four years later undergoing cooperative testing with headphones

The outcome of every clinic visit is recorded in a database at the time, giving us a prospective record of the ENT health of our defined birth cohort over time. For this study, data were extracted from the database for the presence of OME and sleep-disordered breathing (SDB) for every clinic visit, for every child.
The diagnosis of OME is based on a history of hearing impairment, speech delay and sometimes recurrent ear infections, together with otoscopic appearances and tympanometry. When asymptomatic or minimally symptomatic, parental concern is low, speech is developing and soundfield minimal response levels are no worse than 40 dB (approximating to audiometric thresholds of 20 dB), then OME is usually managed by simple observation. Where the OME is associated with significantly elevated hearing thresholds (typically minimal soundfield reponse levels of 45 dB or more) and developmental concerns on the part of parents or professionals, the parents are offered the choice of bilateral grommet (ventilation tube) insertion or hearing aids.
For the purpose of this study, children have been identified as having ‘mild obstructive symptoms’ if the parents give a history of daytime blocked nose, snoring and rhinorrhoea. Those with heavy snoring in association with restless sleep, witnessed apnoeas and snort arousals are defined here on clinical grounds as having SDB. Due to resource limitations, sleep studies are not used routinely. Children with a clear clinical diagnosis of SDB are offered adenotonsillectomy. Children with an uncertain diagnosis of SDB or those who have undergone adenotonsillectomy without resolution of the problem, are referred for full 12-channel Polysomnographic sleep studies.
The prevalence figures shown in Tables 2 and 3 and Figures 3 and 4, were calculated based on age and disease status recorded for each clinic visit, excluding those who failed to attend. Where a child attended twice in a 12-month period, only one visit was included in the analysis to prevent children being included twice in the prevalence figures.
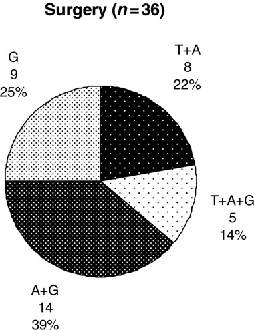
Overall outcome of appointments to the clinic Surgical procedures performed in the study period. G, bilateral insertion of grommets (ventilation tubes); T + A, adenotonsillectomy; A + G, adenoidectomy and grommets; T + A + G, adenotonsillectomy and grommets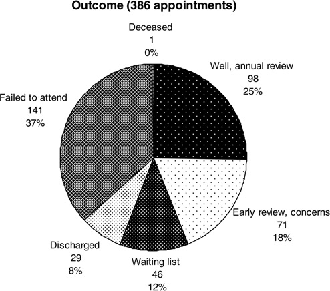
Number of children with Down's syndrome in Greater Glasgow by year of birth
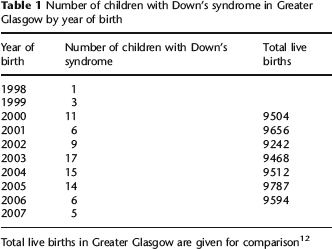
Total live births in Greater Glasgow are given for comparison 12
Prevalence of OME by age
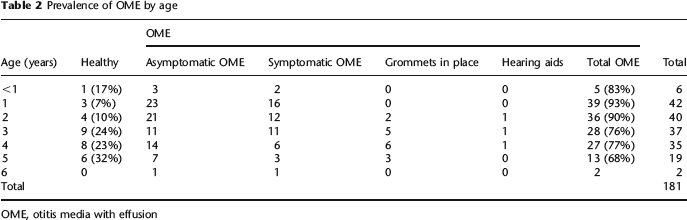
OME, otitis media with effusion
Prevalence of obstructive symptoms by age

T +A, adenotonsillectomy; SDB, sleep-disordered breathing
Results
Since September 2004, 87 children have been identified as having Down's syndrome in Greater Glasgow. Of the 87 children, 48 (55%) were female and 39 were male.
Table 1 shows the year of birth of the children identified. Most children born in 1998 and some born in 1999, would have already started school before our preschool surveillance clinic was established, so only a minority of the children born in those years would have been included in our data. Similarly, not all children born in 2007 will have been seen in the clinic yet. If we exclude those years, and look just at the children born between 2000 and 2006, there were 78 children. Given that there were 66,763 live births in Greater Glasgow over that time period, the number of children seen in our clinic is in accordance with an incidence of approximately 1.16 per thousand live births.
Information was recorded prospectively from all clinics held between 7 September 2004 and 10 September 2008. Over this period of 48 months, 58 clinics were held and a total of 386 appointments were made. For 141 of the 386 appointments, the family did not attend the clinic (37%). However, over the study period 79 out of 87 (91%) children attended at some point and therefore have some data available.
The overall outcome of the clinic appointments is shown in Figure 3. In a quarter of cases the child was well, with normal hearing and no health concerns. Accordingly, a routine annual review appointment was made. Twenty-six children reached school age (5–6 years) and were therefore discharged from the community clinic to be followed up in school. Three children moved out of Greater Glasgow and were also discharged, with arrangements for follow-up in their new area of residence. Four children moved into Glasgow from elsewhere over the same period, so the overall number of children with Down's syndrome has remained relatively stable. One child with severe congenital heart disease died during the study period. At 71 of the appointments, the child was found to have ENT health problems that were not severe or persistent enough to require immediate surgery, but which were of enough concern for an early review appointment to be made. These health problems usually consisted of either OME with mild hearing impairment, or obstructive upper airway symptoms not severe enough to be diagnosed as SDB.
Forty-six of the appointments (12%) ended in the child being added to the waiting list for surgery or investigation. Of these, 10 children were referred for Polysomnographic sleep studies, while on the remaining 36 occasions, the children were listed for surgery (Figure 4). For 13 children, surgery included adenotonsilectomy for SDB. For 28 children (including 5 undergoing adenotonsillectomy for obstructive symptoms), surgery included the insertion of grommets for OME. In addition, six children had evoked response audiometry performed because of difficulty obtaining reliable behavioural hearing thresholds, and this was done under the same anaesthetic as ventilation tube insertion. Seven children underwent more than one surgical procedure. In each of these cases, the second procedure was for re-insertion of grommets that had been naturally extruded. Over the study period, 29 out of the 79 (37%) children who were seen in the clinic were listed for surgery at some point.
OME is highly prevalent in our study population. It can be seen from Table 2 and Figure 5 that 93% of one-year-olds had OME, although not all were symptomatic or needed treatment. By school entry, the prevalence had fallen to 68%. It can be clearly seen in Figure 3, that only a minority of children with OME had symptoms of sufficient severity to require intervention. Although hearing aids were discussed as an option whenever OME was symptomatic enough to require treatment, only four families opted for hearing aids. In one case this was the only treatment used, while one other went on to have ventilation tubes instead, due to difficulties with hearing aid fitting and tolerability (and therefore does not appear in Table 2). In two cases, the family opted for grommets first, but then went on to use hearing aids afterwards because narrow ear canals meant that only very short-lived grommets could be inserted (mini-Shah grommets) and the period of benefit from surgery was consequently very short. Five children (24%) of the 21 with grommets, at some time had short-lived episodes of otorrhoea, but all quickly settled with topical antibiotics and ventilation tube removal has not yet been required. No child in our preschool population has yet been identified to have a sensorineural hearing impairment or a residual hearing impairment with grommets in place. Equally, none has yet developed tympanic membrane atelectasis, chronic perforation or cholesteatoma.
Prevalence of otitis media with effusion (OME), by age, based on the data in Table 2. ‘symptomatic OME’, OME in association with significant hearing impairment and parental/professional concern; arrangements made for ventilation tube insertion or hearing aid provision; ‘asymptomatic OME’, OME without significant hearing impairment or concern; arrangements made for early clinical review only; ‘healthy’, no evidence of OME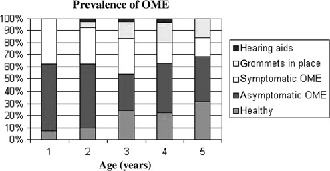
Obstructive symptoms are also very common in our study population (Figure 6). The proportion with a prior history of adenotonsillectomy for obstructive symptoms obviously accumulates with time, but the proportion of the remainder with obstructive symptoms at any one time, remains fairly constant at around 40% (Table 3). Since those with clear SDB all go on to have adenotonsillectomy, it is clear that a significant number of children are developing new obstructive symptoms each year. By the age of five years, 79% have either had adenotonsillectomy or have ongoing obstructive symptoms. Adenotonsillectomy proved to be very efficacious in this population and none of the children seen, has gone on to need continuous positive airways pressure or tracheostomy for ongoing obstructive sleep apnoea. Two children with persistent sleep disturbance after adenotonsillectomy, went on to have Polysomnographic sleep studies and neither of these showed any significant evidence of upper airway obstruction.
Prevalence of upper airway obstructive symptoms, by age, based on the data in Table 3. ‘previous T + A’, previous adenotonsillectomy for obstructive symptoms; ‘SDB’, clinical evidence of sleep-disordered breathing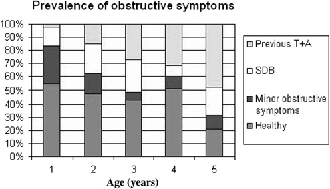
Other ENT problems found in this population were congenital torticollis (1 case), laryngomalacia (1 case) and symptomatic congenital subglottic stenosis (2 cases), all of which had already been identified in infancy before the child attended the surveillance clinic. One child was referred from our clinic on suspicion of autism, due to his behaviour on hearing testing. The diagnosis was subsequently confirmed.
Discussion
This is the first study to provide detailed prevalence data by age for OME and obstructive symptoms in preschool children with Down's syndrome. The high prevalence figures for these conditions would lend support for the idea of regular health surveillance in these children, and for the close involvement of ENT surgeons in particular. Even though a large number of patients failed to attend for appointments (not unusual for community-based clinics in our area), the large proportion of children seen who went on to have surgery and other interventions, suggest to us that this is a good use of a surgeon's time. The multidisciplinary nature of the clinic means that all the necessary professionals are present (education, audiology, ENT) ensuring excellent communication and joint decision-making.
Our study can be criticized for not using objective measures for diagnosis in every case, relying instead on the assessment of an experienced clinician. This reflects real clinical practice. Faced with a child who has clear evidence of SDB, it has been our preference to proceed straight to surgery and avoid any delay waiting for a sleep study. Polysomnography is a limited resource that we reserve for those with an unclear history or persistent symptoms. It is possible, therefore, that our figures underestimate the prevalence of SDB, since mild degrees may go unnoticed by parents. Similarly, evoked response audiometry is only used in our practice when behavioural hearing testing is inconclusive.
Of interest is the low prevalence of autism, sensorineural hearing impairment and chronic otitis media (perforation, cholesteatoma and atelectasis) compared with other studies. It should be noted that our study is unusual in including only the youngest children (aged 1–6 years) in whom these conditions are uncommon. Our own experience, in keeping with the published literature, is that these conditions are not uncommon in children with Down's syndrome as they get older, but that they are rarely seen in the preschool age group.
There has been considerable debate about the merits of surgical intervention in children with Down's syndrome. Adenoidectomy produces less of an improvement in nasal symptoms and in ear health in children with Down's syndrome than it does in other children, 13 but that is not to say it is not worthwhile. It still produces a significant improvement in symptoms in a large proportion of children. Even though the adenoids and tonsils may be small, their removal in children with evidence of SDB can lead to significant improvement in airflow and sleep quality.14–16 Some children, particularly those with associated cardiac anomalies, may require more aggressive surgery such as tracheostomy, but the majority of children with SDB and Down's syndrome should undergo adenotonsillectomy before anything more major is considered. It is well-known that the incidence of otorrhoea after grommet insertion is high, 17 but our experience has been that the infections can be adequately controlled with antibiotic ear drops and grommet insertion still provides worthwhile improvement in hearing. The alternative, of course, is hearing aids but these also have their problems. The narrow ear canals found in Down's syndrome make hearing aid fitting difficult due to wax impaction and acoustic feedback, and children with behavioural problems may refuse to wear aids altogether. The ideal approach is to have both grommets and hearing aids available and to tailor the treatment to the needs of the child.
Thirty-seven percent of children were listed for surgery as a result of clinic visits. While it might be tempting to attribute this to an over-aggressive surgeon, the same surgeon listed only 27% of children from general ENT clinics over the same time period. This would suggest that there genuinely is a significant excess of pathology in the cohort with Down's syndrome.
We are not the first group to suggest an aggressive approach to the management of ENT problems in preschool children with Down's syndrome,18,19 although we are the first to do so in conjunction with a community-based surveillance programme. Because of their pre-existing learning difficulties, children with Down's syndrome can be affected much more than typically developing children when they have a mild hearing impairment or chronic sleep disturbance, and this is especially so when these problems occur during the important early years of development. Surveillance is worthless if it does not also lead to early intervention. We believe that early aggressive management of hearing and sleep problems can lead to sustained improvements in educational attainment for these children, although only time and further evaluation will show if this is correct.