
Abstract
The ability to acquire surgical skills requires consistent practice, and evidence suggests that many of these technical skills can be learnt away from the operating theatre. The aim of this review article is to discuss the importance of surgical simulation today and its various types, exploring the effectiveness of simulation in the clinical setting and its challenges for the future. Surgical simulation offers the opportunity for trainees to practise their surgical skills prior to entering the operating theatre, allowing detailed feedback and objective assessment of their performance. This enables better patient safety and standards of care. Surgical simulators can be divided into organic or inorganic simulators. Organic simulators, consisting of live animal and fresh human cadaver models, are considered to be of high-fidelity. Inorganic simulators comprise virtual reality simulators and synthetic bench models. Current evidence suggests that skills acquired through training with simulators, positively transfers to the clinical setting and improves operative outcome. The major challenge for the future revolves around understanding the value of this new technology and developing an educational curriculum that can incorporate surgical simulators.
Introduction
Rising demands on current surgical programmes have led to investigations into new approaches to training. 1 The ability to acquire surgical skills requires consistent practice, and evidence suggests that many of these technical skills can be learnt away from the operating theatre. 2 Surgical simulation is one of the methods through which surgical education has focused in the last few years. It offers the opportunity for trainees to practise their surgical technical skills prior to entering the operating theatre, allowing detailed feedback and objective assessment of their performance. 1
Simulation can be defined as the reproduction of the essential features of a real-life situation. The aim of simulation is to represent reality as close as possible such that the trainee is convinced the simulated encounter replicates what would happen in a real-life situation. 3 Surgical simulation has evolved considerably over the past two decades and is now a mainstay in training, playing a major role in the acquisition of new skills and knowledge outside of the clinical environment. 4 It is considered particularly valuable in the surgical discipline because it avoids the use of patients for skills practice, ensuring that surgical trainees have had sufficient practice before permitted to treat humans.1,5 Gallagher et al. suggest that simulation-based surgical training allows an individual to acquire technical skills to the point where many psychomotor and spatial judgement skills become ingrained and automated. 6 This places the trainee in better stead to manage intraoperative complications rather than refining technical skills during real-life scenarios.1,6
The aim of this review article is to discuss the importance of surgical simulation today and its various types, exploring the effectiveness of simulation in the clinical setting and its challenges.
The need for surgical simulation
Surgical training consists of developing cognitive, clinical and technical skills, where the latter is traditionally acquired through mentoring. 7 Apprenticeship models were developed over a century ago, originally championed by Dr William Halsted in 1904. 4 The Halstedian model describes gaining progressive experience through supervised training on patients, but this depends on an opportunistic flow of patients in the operating theatre and precludes any organised curriculum.8,9 There is a need to adopt a more formal skills-based training programme. Surgical simulation provides the opportunity for self-directed learning through continuous evaluation and feedback, permitting the trainee to correct deficiencies in training and performance.1,10
With the implementation of the new European Working Time Directive (EWTD) in the National Health Service (NHS), trainees are beset with restrictions in working and training hours. Before the EWTD, a trainee could expect to work over 30,000 hours between becoming a basic surgical trainee and becoming a consultant surgeon. Chikwe et al. 11 have reported that this will now fall to a mere 6000–8000 hours, based on calculations by the Royal College of Surgeons. Coupled with an increasing number of patients presenting with serious and complex surgical problems, this translates to young surgeons required to be more proficient albeit decreased mentoring opportunities. 12 The use of simulators alleviates the burden placed on trainees for developing core skills, in light of shortened clinical and operative opportunities.
Continuous quality improvement is imperative to health care services. The use of surgical simulation enables better patient safety and standards of care.13,14 Innovative state of the art simulation devices can train both surgical tasks and skills without risk to patients. This allows for the detection and analysis of errors and ‘near misses’ which are potentially avoidable. 15 During early training, surgical trainees should be closely supervised, but it is inevitable that preventable patient injuries may occur due to inexperience. In the clinical setting, such errors must be prevented or terminated immediately by supervisors in order to protect patients.13,14 In a simulated environment, however, training errors can be allowed to progress in the face of error. 14 This allows trainees to be taught the implications of the error, and reactions to rectify such deviations. The availability of video feedback for many surgical simulators, strengthens the impact of learning and provides further incentives for behaviour modification.13,14 A study by Fried et al. 15 has also shown that the use of an Endoscopic Sinus Surgery Simulator (ES3) for training surgical residents, when amalgamated with a rigorous formal curriculum, inculcates a unique culture of safety into participating surgical training programmes. They believe a structured curriculum incorporating surgical simulation will improve surgical efficacy, reduce errors and ultimately improve standards of safety in surgical departments. 15
Additionally, the operating theatre no longer serves as the ideal atmosphere for the training of novice surgeons. 16 Ethical concerns about teaching and learning surgical skills on live human patients have been voiced. 17 With simulation, trainees have their first encounters with real patients when they are at higher levels of technical and clinical proficiency. Existing practitioners can also use surgical simulation to improve proficiency when learning new procedures or when honing existing skills. 14
Types of surgical simulation
A wide host of simulation models and devices now exist for the benefit of trainees. 1 Many academic medical centres and University hospitals have developed skills laboratories to accommodate learners through a range of surgical specialties, allowing them to practise their skills. 18 Surgical simulation enables repetitive performance of a single task to allow a trainee to develop essential hand–eye coordination and motor skills prior to entering a real-patient setting. 1 Through surgical simulation, the development of speed, efficiency and precision are honed through continual practice. Eventual automaticity and proficiency in the skill can thus be achieved. 19
As surrogates for human anatomy, surgical simulation laboratories rely on a variety of bench model simulators. These models differ greatly with respect to their degree of fidelity or ‘realism’ to live patients. 16 They can be divided into organic or inorganic simulators. Organic simulators, consisting of live animal and fresh human cadaver models, are considered to be of high-fidelity. Unfortunately, studies have shown that they are limited in terms of availability, high costs, potential for transmission of infectious disease and possible ethical concerns.16,20,21 Lower-fidelity inorganic bench models, on the other hand, often sacrifice realism for the convenience of portability, lower costs and the potential for repetitive use.16,20,21
Inorganic – synthetic
Synthetic simulators are models made of plastic, rubber and latex. They are particularly useful in teaching and learning basic surgical and technical skills, and have been incorporated into courses such as the Basic Surgical Skills Course, in line with the Royal College of Surgeons.
10
Lower-fidelity simulators usually compose of simple devices used for knot tying and suturing techniques. A box trainer is often used in tandem with such simulators, where actual instruments and optical systems used clinically are employed to manipulate the synthetic tissue.1,15 The greatest benefit of such synthetic simulators is the development of hand–eye coordination and motor skills requisite for specific tasks such as cutting, suturing, grasping or clipping structures.
10
Higher-fidelity synthetic models (Figure 1) are more expensive, some of which replicate an entire operation such as aneurysm repair, fracture fixation or femoral-popliteal bypass.
10
TraumaMan® reproduced with permission from Simulab – a life-like, high-fidelity model used to teach basic surgical skills
Inorganic – electronic
With the advent of technology, virtual reality (VR) or computer-based simulation has become increasingly popular due to the high fidelity and haptics (tactile feedback) of the models.
10
VR is defined by Moorthy et al. as a collection of technologies which allow people to interact efficiently with three-dimensional deformable computerized databases in realtime, using their natural senses and skills.22,23 VR simulators (Figure 2) use computer-generated images of organs or objects integrated with a human-computer interface. This allows the trainee to manipulate the images and obtain objective feedback on his performance from the computer.
22
Captured virtual reality endoscopic simulator pictures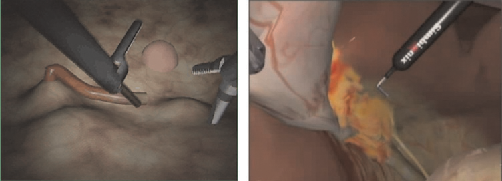
Currently, both laparoscopic and endoscopic surgeries, as opposed to open surgery, have received most of the development focus in surgical VR simulators.1,24,25 This is mainly attributed to the fact that laparoscopic and endoscopic scenarios are more easily recreated by VR simulators rather than open surgery, as they comprise a two-dimensional visual system without much haptic interactions.1,26 Their increased emphasis also stems from efforts to address complications and problems identified in early clinical experience with laparoscopic cholecystectomy. 27 Studies have shown that VR simulators are useful and effective in the training of procedures such as upper endoscopy, flexible sigmoidoscopy and colonoscopy.28–32 Within the last few years, there have been developments in other VR simulators for minimizing invasive gastrointestinal surgery. These systems are of higher fidelity and have improved haptics, examples of which include the Reachin®, ProMis® and LapMentor®. VR simulators are appealing but are often limited due to high costs.
Hybrid simulators combine both attributes of physical simulators and VR simulators, often taking the form of a mannequin linked to a sophisticated computer programme which provides visual images or feedback.1,33 The computer programme can simulate physiological and physical responses such as bleeding, as a reaction to a procedure. These simulators allow the production of a realistic clinical environment where team-working is reinforced, bridging gaps in the operating theatre.1,34
Organic – animal
Anaesthetized, live animals provide a high-fidelity environment which allows trainees to develop psychomotor and cognitive skills necessary for the operative setting.1,35 The advantage of animal models is that they allow trainees to work together as a team on a live operation through reinforcing team relationships, communications and gradients of authority.1,34 They have been used extensively in both open and laparoscopic surgical training, the most common animals being canine, porcine and baboon models.1,36,37 Examples include the use of the dog in the coronary bypass model where it was shown that vascular trainees improved their technical complications rate. 10 However, anatomy of animal models differs from humans. The Calot's triangle in pigs varies from that in humans, so laparoscopic cholecystectomy in these animal models should not be confused. 10 Animal models are most commonly used in Europe and America. Currently, the UK law forbids the use of live animal tissues for practising of surgical techniques due to ethical issues but allows the use of dead animal tissue. Sheep and pig skin are commonly used for bowel anastomosis in surgical courses. 10 Although these animal models provide very realistic haptic feedback, they are limited by high costs and the need for more sophisticated training, such as perioperative monitoring and analgesia of the animals. 1
Organic – cadaver
The main advantage of cadaveric training is the acquisition a detailed understanding of human anatomy and its relations to diseases.1,38 Cadaveric procedures commonly practised on by trainees include laparoscopy, endoscopy and saphenous vein cutdown.39–41 Cadavers are used commonly in America, as well as in the UK, for certain courses such as the Definitive Trauma Skills Course. 10 Unfortunately, cadavers preserved by formalin lose some fidelity as a surgical instructional model. Its high cost and single use have also limited its supply to many medical schools, decreasing opportunities for dissection. 38
Assessment of competency
Simulation holds a strong common-sense appeal. Nevertheless, attractive programmes are not inherently sufficient. 42 We need to know if they can work, and if they can assess true surgical competency. 42 Ideally, assessment should produce reliable and valid results which are both affordable and practical for the trainee and institution. 43 Assessment results should also correlate with the trainee's actual operative experience and must be shown to improve with surgical training, distinguishing between experienced and novice surgeons. Discussed below are some of the objective methods currently used to assess competency with surgical simulation. 43
Motion analysis systems
The Imperial College Surgical Assessment Device (ICSAD) was developed at Imperial College, London.43,44 The system consists of a commercially available electromagnetic tracking system connected to a portable computer. 10 The device's electromagnetic trackers and two sensors are affixed to the dorsum of the trainee's hand, and bespoke software is used for the retrieval of data and analysis. 10 ICSAD gauges positional data to produce dexterity measures of the trainee, such as distance travelled, number and speed of hand movements and time taken to complete the task. 44 Recently, Dosis et al. have developed a new software known as ROVIMAS – Robotic Video Motion Analysis Software. 45 This enables video integration on the ICSAD, where the user can concentrate on video frames exhibiting kinematic properties which can result in operative errors.10,45 Other studies have validated the construct of ICSAD with respect to a range of laparoscopic tasks. 10 Experienced and skilled laparoscopic surgeons exhibit more economical movements, hence use significantly lower path lengths which is a determinant or accuracy. 10
Virtual reality
The minimally invasive surgical trainer-virtual reality system was one of the first commercially available VR laparoscopic simulators. 10 The system was developed in collaboration with surgeons and psychologists, who designed a task analysis of laparoscopic cholecystectomy. A particularly attractive feature of VR simulation is its ability to generate output data, or what is known as metrics. This allows objective and repeated measurements of the activity performed, such as the time taken to complete a task, the errors made in the process and also the economy of movements in the accomplishment of the task. 1 Realtime feedback can be provided, and results compared with validated data. The use of metrics also allows the opportunity for assessment of competency without the need for an observer to be present. VR trainers can allow trainees to practise independently in their free time, and this can be incorporated into a structured curriculum.1,34 A large proportion of surgical VR systems function as part-task trainers, which focus on the training of a particular task within the surgery, that aims to improve the quality of surgery by shaping certain skills required to perform the surgery. 1
Task-based analysis assessment
This type of assessment of technical skills is derived from human error and reliability analysis. It breaks down an operation into fundamental/key steps and these key steps are then broken down into mini steps. The key steps are very important in the quality of the operation, while the mini steps incorporate more generic technical skills, e.g. knot tying, haemostasis, etc. Sarker's group10,46–49 has demonstrated the construct validity and reliability of this method of assessment over the past few years in endoscopic, open and intermediate and advanced laparoscopic surgery.
Effectiveness of simulation
To establish a benefit in using simulated environments to teach surgical skills, it must be shown that skills acquired through training with simulators can positively transfer to clinical practice, translating into better patient outcome. 1 Recent evidence does suggest an improved performance in clinical setting after the use of simulation. Scott et al.16,50 demonstrated that surgical residents who underwent laparoscopic skills training with a simulated video trainer exhibited significantly improved performances on laparoscopic tasks in the operating room, as compared with the control group who was not exposed to any training. In addition, other disciplines have also established the value of simulation in the clinical setting. Naik et al. report that fibreoptic orotracheal intubation skills acquired by anaesthesiology trainees on a simulator, translated into better performance on real life-patients. They were compared with trainees who received didactic teaching only, and both groups were evaluated by blinded anaesthesiologists who found that the simulation-trained group significantly outperformed the control group. 51
A recent meta-analysis by Haque et al. analysed 16 prospective and randomized studies for the training effectiveness of VR surgical simulators. Their results showed VR simulation training was highly effective in the transference of skills from the simulation environment to the operating room, while being able to discriminate between the experienced and inexperienced trainees. 52 The VR trained group took significantly less time for task completion, compared with the control groups in the process. These results are indeed promising, but further prospective trials are required to explore the nature and duration of simulation training required to deliver the greatest clinical benefits.
Although simulation in surgery holds much promise for the future and serves as an invaluable resource to the education of young surgeons, it is not a one-stop solution to our training needs. Becoming a competent surgeon requires the amalgamation of good patient communication, team-work within a multidisciplinary setting, leadership skills, decision-making and clinical acumen. Technical skills are just one aspect of the myriads of competencies required of a surgeon. We believe that apart from VR systems, it will be prudent to engage as many members in the operating theatre during simulation, to re-enact the actual ‘live’ setting of operating. This will enable key decision-making skills to be developed and foster team-based environment which will improve effectiveness of simulation.
The challenge
The discussion thus far has concentrated mainly on the acquisition of skills through surgical simulation and the pros and cons of each system.
42
It is imperative to consider how to assimilate simulation into training. Satava,
33
a VR pioneer has said, ‘simulators are only of value within the context of a total educational curriculum, and technology must support the training goals. New technology must continually seek to improve the quality of teaching and learning, and not simply to open up access to new information and experiences.
42
Managing simulator-based learning, as described by Kneebone,
42
should be an active process properly embedded in the learning context of the institution. Simply providing sophisticated equipment will not guarantee a successful learning outcome or translate into better patient outcomes.33,42 At present in the UK, there is no surgical programme that rigorously incorporates surgical simulation into the assessment and training of surgeons. The major challenge, therefore, revolves around understanding the value of this new technology, and developing an educational curriculum (Figure 3) that can incorporate surgical simulators.
Proposed curriculum of assessment and feedback for the higher surgical trainee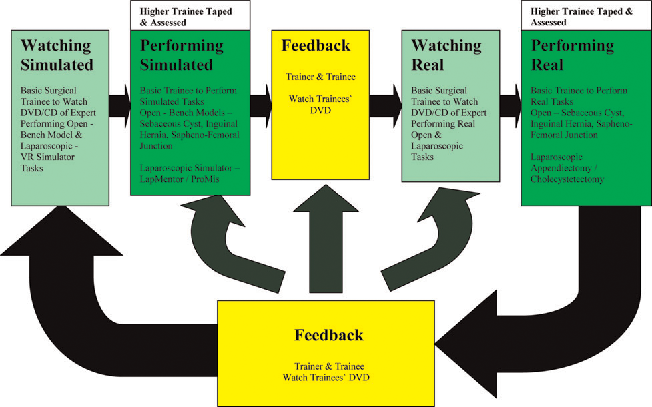
Conclusion
With rapid advances in technology and the adoption of more minimally invasive surgical interventions, there is a demand for more simulators to complement and provide training. Simulator-based learning, commands an enormous potential and seems poised to revolutionize surgical training in future. 42 For this to succeed, more studies will need to validate the translational benefits from simulation to the operating theatre and identify skills that are developed the most with simulation. Currently in the UK, only certain medical schools have a dedicated surgical simulator centre. We believe that for simulation in surgery to succeed, this will require academic directors in surgery to embrace the potential of this technology and actively promote it. A rigorous educational curriculum incorporating surgical simulation will augment the operative exposure of surgical trainees, improving current training standards and its research.
Footnotes
Conflict of interest
We declare that we have had no inappropriate influence in our work, which includes avenues from employment, consultancies, stock ownership, honoraria, paid expert testimony, patent applications/registrations, grants or other funding. We declare that these do not pose a conflict of interest with regard to the submitted manuscript.