
Abstract
Colonic atresia (CA) is an unusual cause of neonatal intestinal obstruction where a section of the colon has failed to form, leading to blockage or absence. A premature baby was delivered at 32 weeks of gestation via caesarian section following fetal distress. She was grossly oedematous and diagnosed with severe fetalis hydrops secondary to anaemia. She was resuscitated and stabilized. On the sixth day of life, the neonate's abdomen became severely distended with bilious vomiting and failure to pass meconium. We suspected intestinal obstruction and performed an omnipaque enema which revealed dilated small bowel loops and a bowel atresia. Exploratory laparotomy confirmed a Type 1 Bland Sutton CA with mucosal web. An end colostomy was successfully performed and uneventful. In our case report, we describe a rare occurrence of postnatally diagnosed CA, complicated by fetalis hydrops and anaemia.
Introduction
Colonic atresia (CA) is a rare cause of neonatal intestinal obstruction, comprising only 1.8–15% of all gastrointestinal atresias. 1 It describes a condition where a section of the colon has failed to form, leading to blockage or absence. Any process that results in occlusion of branches of the superior mesenteric artery or the inferior mesenteric artery, may result in atresia. It is commonly associated with intrauterine mesenteric vascular obstruction caused by intestinal hernia, intussusception or volvulus. 2 We present a novel case of postnatally diagnosed CA, complicated by fetalis hydrops and anaemia. Consent was obtained from the patient's parents.
Case report
A 32-year-old Chinese woman, Gravidity 2 Parity 1, delivered a female neonate at 32 weeks’ gestation. She had no significant past medical history. She had a previous normal vaginal delivery of a live female baby three years ago, with a birth weight of 3210 g. Her earlier antenatal scans were also normal. At 32 weeks of gestation, she presented to our institution with signs of fetal distress. On ultrasound, the fetus was cephalic and her amniotic fluid volume was 37 cm showing polyhydramnios. There was the presence of pleural effusion and massive subcutaneous oedema in the fetus with minimal pericardial effusion and ascites. An MCA Doppler ultrasound was performed which had a maximum of 93.8 cm/second (2.22MOM), showing severe anaemia in the fetus.
She was subsequently put on continuous cardiotocography monitoring. An intramuscular dexamethasone injection was also administered. Her toxoplasma, rubella and cytomegalovirus screens, Parvovirus B19 as well as the Kleihauer's test were all negative. Her immunoglobulin G anti-B titre was 128 units. She underwent an emergency lower segment caesarean section, and delivered a female neonate with a diagnosis of hydrops fetalis not due to isoimmunization.
The neonate weighed 2847 g at birth and had Apgar scores of 3 and 7 at one and five minutes, respectively. At birth, she was grossly oedematous with no spontaneous respirations or movements. She was subsequently cling-wrapped and intubated. The working diagnosis was severe fetalis hydrops secondary to anaemia (Hb 8.4g/dL). Over the next five days, she was given three doses of packed cell transfusion and platelet infusions. Chest drains were inserted for her bilateral pleural effusions. She was also intubated with two doses of surfactant for her respiratory distress.
On the sixth day of life, the neonate's abdomen became extremely distended and a hepatomegaly of 3 cm was noted. Paracentesis was performed and the ascitic fluid was drained. There was also one episode of a large amount of bilious vomiting after feeding. These led to the suspicion of intestinal obstruction and an omnipaque enema was performed. The enema revealed obstruction at the mid-proximal level of the sigmoid colon, with dilated small bowel loops (Figure 1). These findings were in keeping with proximal bowel atresia and the patient subsequently underwent exploratory laparotomy.
Omnipaque enema performed revealing dilated small bowel loops
At laparotomy, there were findings of a straw-coloured peritoneal fluid. The descending colon, in the distribution of the inferior mesenteric artery, was noted to be atretic. Her proximal small bowel displayed marked dilation and congestion. Distally, there were no other obstructions or mesenteric defects, although there was a microcolon appearance (Figure 2). There was a well-demarcated cut-off between the atretic and proximal small bowel. Visible pulsations were also noted in the inferior mesenteric artery. These findings suggested a Type 1 Bland Sutton CA with mucosal web and the serosa was in continuity. The atretic part of the descending colon was mobilized and resected, containing a 2 cm segment (Figure 3). The junction between atretic and normal bowel was ligated, excised and sent for histology. An end colostomy was successfully performed and uneventful. The histology reports were consistent with the diagnosis of microcolon with atresia.
Operative findings of a microcolon and proximal dilated small bowel Resected segment of atretic descending colon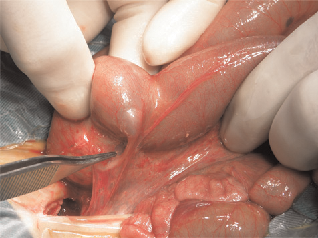

Discussion
There have been no published cases of CA co-existing with Hydrops. The incidence of associated anomalies is much lower in cases of CA as compared with other atresias. 1 It has previously been associated with abdominal wall defects and abnormalities of the genitourinary tract, where reported associations include Hirschprung's disease and Gastroschisis. 2
CA is fatal should the obstruction persist. Complications such as dehydrations, electrolyte imbalance, acidosis and sepsis can quickly occur if the problem is not addressed. 3 The problem with CA is that the diagnosis is often delayed until after several feeds, and only when abdominal distension, vomiting and failure to pass meconium are observed. 1 Our neonate is an example of late diagnosis occurring on her sixth day of life. Antenatal ultrasound scans did not reveal any characteristic features of CA, and her birth was complicated with fetalis hydrops.
Fetalis hydrops is a clinical condition where there is excessive fluid accumulation in the extravascular compartment of the fetus, leading to widespread soft tissue oedema and collection of fluid in the fetal body cavities. 4 Our neonate was diagnosed on antenatal ultrasound scans at 32 weeks, with the presence of massive skin oedema around the fetal head and neck area, pleural effusion and ascites. Immune hydrops fetalis was ruled out as blood tests did not reveal any rhesus iso-immunizations. Her hydrops was believed to be secondary to anaemia, as her blood results showed decreased haemoglobin levels (8.4 g/dL). As this was an emergency situation, the focus of the preliminary management was resuscitation and stabilization of the neonate. Drainage of her pleural effusions was performed in order to prevent pulmonary hypo-plasia and a paracentesis was also performed to drain her ascites.
Rennie 5 has described that hydrops may develop because of decreased intravascular colloid osmotic pressure. Protein is lost as a transudate into the bowel or there could be abnormalities of lymphatic drainage in the splanchnic bed. In our neonate, paracentesis was performed which revealed an abnormally high protein content of 24 g/dL. We suspect that there could be a correlation between her hydrops and increased protein transudate caused by obstruction in the atretic segment, leading to dilation of her proximal bowel. This culminated in interference to the mesenteric blood supply.
The diagnosis of CA in our neonate was based on clinical and radiological findings. She presented with symptoms typical for obstruction which included abdominal distension, bilious vomiting and failure to pass meconium. On omnipaque enema there was presence of air fluid levels, a disproportionately dilated loop of bowel as well as a ‘wind-sock sign’ where the intraluminal membrane balloons into the dilated proximal bowel. 1 These are pathognomonic of CA. There has been a dilemma whether primary anatomosis or a staged operation is indicated in the management of CA. Primary anastomosis was technically difficult because of the large discrepancy in the size of the distal and proximal bowel. Moreover, there is the possibility of early anastomotic leak. In our neonate, due to her medical history complicated with hydrops, we decided on the staged approach with colostomy. This allows treatment of her immediate problems caused by hydrops before subsequent anastamosis when her condition becomes more stable. At the time of writing, our patient was recovering well following her colostomy without any postoperative complication.