
Abstract
Ultrasonography has been used to detect fetal congenital heart disease since the 1980s, although there has been little uniformity in policy. In the UK, data published for 1993-1995 found an average detection rate of 23.4% with a Scottish rate of 9.6%. At the time of this study, 10 out of the 14 health boards in Scotland were implementing the 16-22-week fetal anomaly scan (FAS). The aims of this study were to determine the rate of antenatal diagnosis of major congenital heart disease (MCHD) throughout Scotland during 1 January to 31 December 2006, to document the regional differences in detection and to determine if implementation of a FAS significantly improved rates. Retrospective data were collected from the centralized Paediatric Cardiac Services in Edinburgh and Glasgow. The database contains information on all infants with cardiac disease in Scotland. All infants requiring cardiac intervention or dying in the first year of life were included. The results showed that the antenatal diagnosis rate for Scotland was 28% (95% CI 21.2%, 34.9%). The Scottish health boards that had implemented the FAS had a significantly higher antenatal detection rate (χ2 test P = 0.037). In conclusion, antenatal detection rate of MCHD varies widely throughout Scotland. Implementation of the FAS has made a significant difference to antenatal diagnosis
Introduction
Congenital heart disease (CHD) is the most common form of congenital anomaly 1 and a major cause of mortality and morbidity in the perinatal period. 2 Approximately eight of 1000 babies are born in the UK each year with CHD, and three of 1000 live births are considered major congenital heart disease (MCHD).1,2 MCHD is defined as necessitating surgical intervention or resulting in death in the first year of life 3 and classified according to the International Statistical Classification of Disease and Related Health Problems 10th Revision. 4 Hearts with multiple lesions are classified according to the lesion most important for longterm prognosis. 5
Ultrasound scanning
The potential for detection of fetal CHD using ultrasonography was recognized in the early 1980s.5,6 At 18 weeks’ gestation, all the cardiac connections can be seen in almost every patient. The four-chamber view is the most basic assessment of the fetal heart and is abnormal in up to 60% of all major malformations. 7 The addition of the ventricular outflow tract view allows for the detection of abnormalities not seen in the four-chamber view, such as tetralogy of fallot and pulmonary atresia7–10 and has been found to increase sensitivity by up to 20%. 7
Regional variation
There are major regional differences in the antenatal detection rate of MCHD. In the Eurofetus study, prospective data were collected from 61 obstetric centres across Europe over a three-year period (1990-1993) and the antenatal detection rate was 28%. 11 During the same time frame (1990-1993), data collected by the Eurocat working group found an average detection rate of 62% in Paris, compared with 6.8% in Glasgow. 12 France has consistently had one of the highest detection rates in Europe, having been the first nation to propose assessment of the fetal heart in obstetric scanning. 13
The largest national survey of UK rates was conducted by Bull in 1999. 3 Data were collected from all 17 paediatric centres between 1993 and 1995, and the average rate of fetal diagnosis was 23.4%, with a detection rate of 25.3% in England and Wales, but only 9.6% in Scotland. These rates applied to all cases of MCHD with inclusion criteria similar to the present study.
A more recent study conducted in Northern Ireland found a detection rate of 27% (73/272) for MCHD. 14
Scottish practice
In 2004, NHS Quality Improvement Scotland NHS QIS published recommendations that all Scottish women, in addition to a 10-13-week scan, should be offered an anomaly screening scan between 18-22 weeks’ gestation. 15 During the time frame of the present study (1 January 2006-31 December 2006), 10 of the 14 health boards in Scotland offered a second trimester anomaly scan. 16
Methods
Study population
All infants with MCHD born in Scotland between 1 January 2006 and 31 December 2006, were included in this study. Retrospective data were collected from the two centralized Paediatric Cardiac Services at the Royal Hospitals for Sick Children, in Edinburgh and Glasgow, which receive referrals from all 14 health boards in Scotland. Together the databases contain information on all infants with CHD diagnosed and treated in Scotland plus information on termination of pregnancy and intrauterine deaths that occur after referral to the units. Heartsuite, a fully integrated patient management system designed specifically for paediatric cardiology and cardiothoracic surgery, was used to access information on individual cases. Where information was insufficient, case-notes were sourced.
Data analysis
Confidence intervals were calculated using the Minitab14 package. In order to determine statistically significant results, the chi-squared test was performed using the statistics package SPSS 14. A probability value of P < 0.05 was considered significant.
Results
The criteria for MCHD was fulfilled by a total of 164 cases born in Scotland between 1 January 2006 and 31 December 2006, resulting in an incidence of 2.9 of 1000 live births. The antenatal diagnosis rate was 28% (95% CI 21.2%, 34.9%).
The average detection rate for the health boards that had implemented the second trimester FAS was 35.4% (29/82) (95% CI 25%, 45.7%). This was significantly higher (χ2 test P = 0.037) than the detection rate for the health boards without the Fetal Anomaly Scan (FAS) (20.7% [17/82] [95% CI 12%, 29.5%]) (Table 1).
Fetal diagnosis rates within different health boards, separated according to fetal anomaly scanning
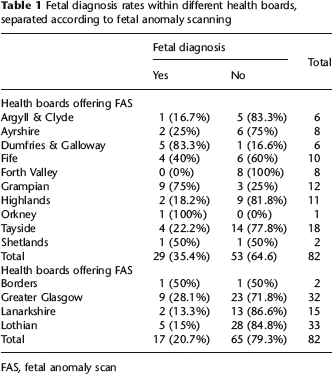
FAS, fetal anomaly scan
The addition of a ventricular outflow tract view to the standard four-chamber view, significantly enhanced anomaly detection rate (χ2 test P = 0.02). The four-chamber view detected 41.9% (26/62) (95% CI 29.7%, 54.2%) of anomalies. Lesions visualized by means of the outflow tract view were detected at a rate of 19.6% (20/102) (95% CI 11.9-27.3%), which increases overall detection rate from 15.9% (26/164) (95% CI 10.3%, 21.4%) (the 4-chamber view alone) to 28% (46/164) (95% CI 21.2%, 34.9%).
Discussion
The antenatal detection rate for MCHD in Scotland during 2006 was 28% (95% CI 21.2%, 34.9%). This is substantially higher than Scottish detection rates of 9.6% as found by Bull in 1999. 3 A recent study conducted in Northern Ireland (2002-2006) found a detection rate of 27% (73/272) for MCHD; this is very similar to the rate found in the present study. 14 However, the detection rate of MCHD in this study is still low when compared with the best European screening programme, as in France.11,12 It is hoped that introduction of FAS across Scotland and enhanced training of sonographers will further improve the detection rate.
Implementation of the FAS in 10 out of 14 health boards resulted in a significantly higher detection rate (χ2 test P = 0.037). This adds to the body of research that has shown an improvement in detection rate following a second trimester scan.10,17,18
The ventricular outflow tract view in addition to the four-chamber view, significantly increases the detection rate of MCHD (χ2 test P = 0.02). This replicates previous studies reiterating that the ventricular outflow tract view increases sensitivity of scanning. 7
This is the first study to report antenatal diagnosis of MCHD for the whole of Scotland since Bull 1999, 3 and thus since the publication of the NHS QIS recommendations in 2004. 15 Results show an increase on previously publicized rates of MCHD in Scotland.3,11,19 There is a significantly higher detection rate for health boards that have implemented the FAS, providing data to support the NHS QIS recommendations. Since 2006, FAS has been or will be implemented in the four remaining health boards, leading to uniformity in Scottish practice and a continued improvement in antenatal detection rates of MCHD in Scotland.
Footnotes
Acknowledgement
I would like to thank Lorraine Leask, Cardiac Services Information Coordinator, Royal Hospital of Sick Children, Dalnair Street, Glasgow G3 8SJ.