
Abstract
Electronic patient health information in secondary care is often stored on different IT systems and not accessible to doctors involved in clinical decision-making. The Scottish Government will support clinical portal implementation in all Scottish Health Boards, which will present information from different sources as a virtual electronic patient record. An online survey was developed and sent to secondary care doctors, who were asked to rank the importance of different types of patient-centred information, knowledge support sources, and information to support appraisal and continued professional development that a clinical portal could deliver. Subgroup analysis was performed to investigate whether expectations differed between senior clinicians and doctors in training. Replies were received from 677 senior doctors and 137 trainees. Patient-centric information such as current medication and allergies, clinical alerts, past medical history, diagnostic test results and clinical letters were ranked as most important. Doctors would also like access to knowledge support, such as clinical guidelines. Eighteen of the top 20 ranked information types were consistent between senior doctors and those in training grades. In conclusion, senior doctors and trainees consistently want to see similar information in the clinical portal which is largely patient-centred with some provision for knowledge support.
Introduction
Secondary care doctors spend a large amount of time recording and viewing clinical information, some of which is stored electronically on a range of local and national IT systems. Even if information is stored digitally, it is usually only accessible to a small number of clinicians within an individual Health Board. Patients usually assume that clinical information is shared with healthcare professionals involved in their care. This is often not the case, leading to clinicians having to make decisions in the absence of adequate information or patients becoming frustrated because they are repeatedly asked to give the same information.
One of the key strategic objectives of the Scottish Government eHealth directorate is to support all Health Boards in Scotland, with implementation of a clinical portal through which clinicians can access the information they need to provide safe and effective clinical care. 1 Portal technology can present clinical information from different sources as a virtual electronic patient record (EPR), without the need for all the information to be stored in a large single database. 2 It is important that the clinical portal programme focuses on delivering benefits to clinicians, even in the early phases of implementation. 3 It was decided to ask clinicians across Scotland, what types of information they felt were important to deliver to them during the early phases of clinical portal implementation.
Methods
An online survey was developed using Survey Monkey,TM which was sent to all Scottish Health Board Medical Directors and clinical eHealth leads, Royal Colleges and national advisory groups, such as the British Medical Association. Each group was asked to send the survey to all clinicians in their Health Board or organization, to try and ensure that all doctors working in NHS (National Health Service) Scotland had an opportunity to complete the survey. In order to capture as many trainees as possible, the survey was also disseminated through the Doctors Online Training System (DOTS) system. The survey was available for completion between 8 May and 19 June 2009.
In the first series of questions, clinicians were asked to rank the importance of availability of different types of patient-centred clinical information, assuming they could be made available through a clinical portal. The second series of questions asked clinicians to rank the importance of availability of performance indicators, knowledge support and information to support audit, appraisal, re-validation and continued professional development (CPD). The final section of the survey asked clinicians about their current access to electronic clinical information. None of the questions were mandatory to complete.
For each question, doctors could rank information as Not Applicable (score = 0), Not Necessary (score = 1), Useful (score = 2), Important (score = 3) or Essential (score = 4). In addition to the questions, clinicians were invited to suggest additional information they felt would be of value, by entering free text comments at the end of each series of questions.
From the results, we conducted subgroup analysis to investigate whether expectations of what a clinical portal should deliver, differed between senior hospital doctors and doctors in training. Senior doctors included professors, consultants, senior lecturers, rural practitioners and associate specialists. For analysis of results in this study, training grade doctors were classified as foundation doctors, specialty trainees, specialist registrars, lecturers and staff grade doctors. Doctors working as general practitioners (GPs) were excluded from analysis.
Data were analysed using an Access database and the mean score for each answer was calculated.
Results
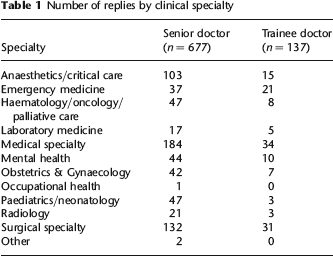
Excluding GPs, 854 doctors completed the survey. Six 4hundred and eighty-five were senior doctors (10 professors, 647 consultants, 26 associate specialists and 2 rural practitioners). One hundred and sixty-nine trainee doctors completed the survey (155 foundation grade doctors and specialty trainees/registrars, 3 lecturers and 14 staff grade doctors). Both groups of doctors came from a variety of specialties (Table 1).
Number of replies by clinical specialty
Both senior clinicians and trainees ranked the same 18 pieces of information in their top 20 scores. Access to diagnostic test results, allergy status, current medication, past medical history and current problem list were the most important items for both groups. The mean scores for general patient clinical information are shown in Figure 1. From the trainee subgroup, the most useful types of clinical alerts were felt to be awareness of Advanced Directives, Do Not Resuscitate orders and Adults with Incapacity forms.

Mean scores (0-4) for patient health summary information
Both groups of doctors thought it was important to have access to laboratory results, as shown in Figure 2. Access to radiology images and reports, and to other diagnostic test reports was felt to be equally important by both groups.

Mean scores (0-4) for diagnostic test results
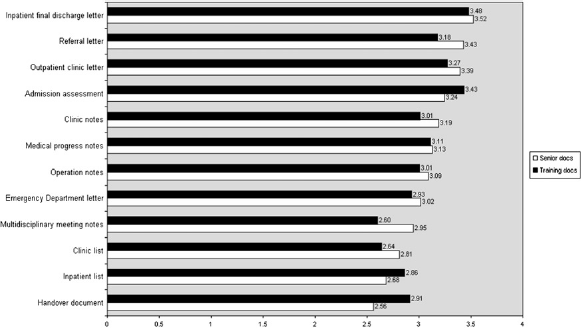
Clinical letters and some types of clinical notes were deemed very important, as shown in Figure 3. The clinical letters with the highest scores, included inpatient discharge letters, outpatient clinic letters and referral letters. Both groups of doctors scored access to hospital admission assessment notes and outpatient clinic notes highly. Providing electronic access to certain types of clinical notes was more important than providing doctors with access to lists of their inpatients or clinic patients. Trainees scored availability of handover notes more highly than senior medical staff.
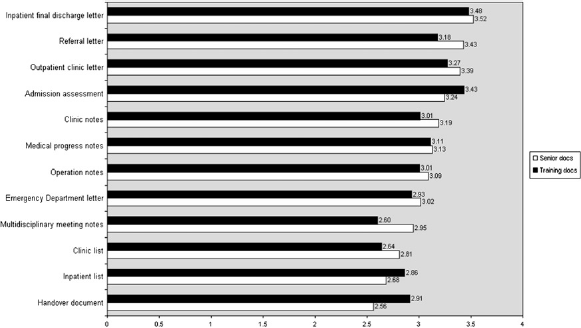
Mean scores (0-4) for clinical letters, notes and patient lists
Both groups ranked access to clinical measurements (e.g. pulse, blood pressure) as important (mean score 3.34 for senior doctors and 3.66 for trainees). Availability of assessment scores, early warning scores and body diagrams were felt to be useful but not important. Assessment scores, such as Early Warning Scores 4 and Mini Mental State Examination, 5 and markers of illness severity, such as Rockall, 6 CURB-65 7 and TIMI scores, 8 were considered to be useful by trainees.
Access to knowledge support including local and national clinical guidelines and resource sources, such as electronic version of the British National Formulary (eBNF), were ranked as important by both groups (Figure 4). Electronic access to other forms of knowledge support was thought to be useful. It was commented that this would be particularly useful if the clinical portal provided single sign-on to existing electronic knowledge support sources. Neither group felt it was important to provide access to performance indicators or tools to support audit, appraisal or Continued Professional Development (CPD). Access to patient-centred information was stated to be more important.
Mean scores (0-4) for knowledge support, performance indicators and tools to support appraisal and continued professional development
Both groups of doctors currently have electronic access to common laboratory results, with 85% of senior doctors and 92% of trainees having access to haematology and biochemistry results. Electronic access to other laboratory test results, such as pathology, immunology and blood transfusion is lower, as shown in Figure 5. At least three-quarters of all doctors had electronic access to both radiology images and reports. Electronic availability of other diagnostic test reports was much poorer, with only 13% of senior doctors and 11% of trainees able to view these digitally.
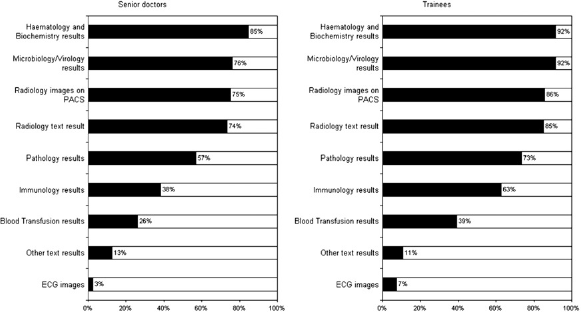
Current electronic access to diagnostic test results and PACS
In both groups, the current level of access to electronic patient health summary information and clinical letters was much poorer (Figure 6). Only 11% of all senior doctors had electronic access to information about a patient's current medication and 7% had access to information about past medical history. The situation was similar for trainees with 13% able to access a medication list and 6% information about past medical history. Electronic versions of hospital discharge letters or outpatient clinic letters were only accessible by a quarter of doctors, while electronic access to referral letters was extremely poor.
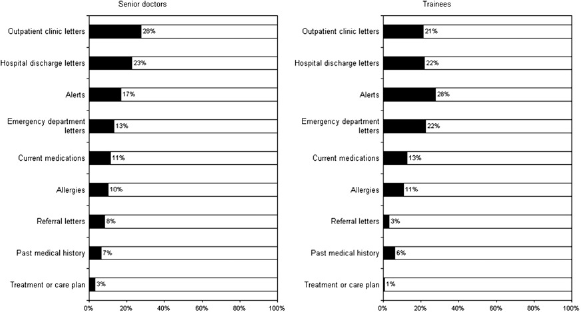
Current electronic access to patient summary health information and clinical letters
Discussion
With the exception of common diagnostic test results, current access to electronic clinical patient information is limited. From our study, less than 15% of all hospital doctors in Scotland have access to information about a patient's past medical history or current medication and the majority of doctors have limited access to clinical letters.
Clinical portal technology will potentially provide the ability for authorized clinicians to view existing electronic clinical information more easily. Within NHS Scotland, two Health Boards have already implemented clinical portal technology to provide users with access to clinical information. 9 In NHS Greater Glasgow and Clyde, a clinical portal was implemented to provide secondary care clinicians in two recently opened ambulatory care hospitals with access to clinical letters, diagnostic test results and patient lists. This reduces the dependency on paper case records and ensures clinical information is available at the point of care. NHS Tayside has also implemented a clinical portal which contains information that is predominantly held in the primary care record, such as medication, past medical history, allergies and alerts. The portal is currently being used in an increasing number of GP practices across Tayside, with a plan to extend access to Emergency Departments in the near future. The national programme aims to support all Health Boards across Scotland, with clinical portal implementation. In the short term, this will ensure clinical information will be available locally to support the safe and effective delivery of clinical care and in the longer term, will improve information sharing across Health Board boundaries.
From our survey, clinicians across Scotland were asked to rank the importance of different types of information that could be made available through a clinical portal. The response rate was high, particularly among senior clinicians. This suggests that they view the implementation of a clinical portal of relevance to them and, from the comments received, they welcomed the opportunity to provide input to this programme of work. The response rate from trainees was lower than might have been expected. While some may have chosen not to respond, the lower response rate may simply reflect inadequacy of the communication channels to this group.
There was a consistent view across both groups that patient-centred information should be made available through a clinical portal. Access to past medical history, current problem list, clinical alerts, allergy status and current medication lists was seen as particularly important. This is in keeping with suggested requirements of electronic health records.10,11 The Emergency Care Summary (ECS) provides some clinicians and pharmacists working in NHS 24, Out of hours services and Emergency Departments with information about currently prescribed medication and known allergies, subject to explicit patient consent to access this information. 12 It is clear from the results that 85-90% of all secondary care doctors who completed the survey are not currently able to view this information.
There was a consensus across both groups that all diagnostic test results should be made available. At the present time, electronic availability of diagnostic test results other than common laboratory tests, or radiology images and results accessible through the Picture Archiving and Communications System (PACS), is very limited. Both groups of doctors would prefer to have text results available initially rather than diagnostic test images, such as electrocardiographs, although this varied by clinical specialty.
Doctors wished to see inpatient discharge letters, outpatient clinic letters and referral letters available in a clinical portal. Availability of hospital admission assessments and clinic notes were ranked as being important by both groups of doctors. Trainees were in favour of electronic handover documents as a mechanism of reducing clinical error and ensuring appropriate timely interventions. 13
Both groups of doctors ranked availability of clinical measurements as being important to deliver through the clinical portal. This is surprising since, in secondary care, there are very few sites where it is possible to record this information electronically at present. There were a number of other clinical assessment tools and scoring systems that were suggested as being useful for trainees. This probably reflects that fact that trainees work across a variety of specialties and it can be difficult remembering specialty specific scoring systems that are important in clinical decision-making.
There appeared to be an interest in using the clinical portal to support safe and up to date clinical practice through the enthusiasm for inclusion of knowledge support sources. Both groups wanted availability of local and national clinical guidelines in addition to resource sources, such as an eBNF, to support practice of evidence-based medicine. 14
Availability of performance indicators and clinical activity statistics were documented as being useful but not important to have available through the clinical portal. This reflected the desire to keep the clinical portal patient-centred. Senior staff ranked critical incident reporting and activity statistics as being more useful than any other form of performance indicator. Trainees did not appear to see any benefit in including performance indicators in the clinical portal. This may reflect a lack of engagement with issues of clinical governance, or simply that senior staff are more likely to use this type of information to support appraisal processes and service redesign.
Neither group thought that information to support appraisal or CPD was important to include in the portal. Trainee doctors were more enthusiastic about incorporation of a record of competencies and logbooks than senior doctors. 15 For trainees, electronic CPD is becoming increasingly ubiquitous and some welcomed inclusion into the portal, with a single sign-on process, to avoid having to use multiple electronic databases. Comments from senior doctors revealed concern that this may lead to a lack of privacy regarding their clinical activities and were keen that this type of activity remained separate from a more patient-centric approach to a clinical portal.
Conclusions
Patients are now being treated on different sites within a health board or across health board boundaries. A virtual EPR is therefore required to promote a seamless transfer of care from one team to another. Our survey demonstrates that current access to such electronic clinical information among hospital doctors is poor and there is a need to significantly improve the availability of this information. There is support from senior and trainee doctors to implement a clinical portal in each Health Board to redress the inequitable access that currently exists. Senior doctors and trainees consistently want to see similar information in the clinical portal, which is largely patient-centred with some provision for knowledge support to improve clinical decision-making.
Footnotes
Acknowledgements
Thanks to Alastair Bishop from Scottish Government eHealth Directorate for his support with data analysis.