
Abstract
Upper gastrointestinal haemorrhage (UGIH) is a common medical emergency. Recent publications have emphasised the need for early risk assessment of patients with this condition to help direct management. Several risk scores have been developed for UGIH and are variably used in clinical practice. In this article, we discuss the various risk scoring systems for this condition and summarise the available evidence for their use.
Introduction
Upper gastrointestinal haemorrhage (UGIH) remains a common cause of admission to hospital. Patients present with haematemesis, coffee ground vomiting or melaena. The UK annual incidence is 103-172/100,000 adults.1,2 Some of the highest reported incidence figures for UGIH have come from Scotland,2,3 which may be partly explained by the increased deprivation and helicobacter prevalence here.
Although a proportion of patients presenting with UGIH require transfusion, endoscopic or surgical intervention and a small minority die, the majority do not require intervention and remain well. Similar to other common medical conditions including chest pain, deep venous thrombosis and chest infection, risk-scoring systems for UGIH have been developed. These are particularly useful in identifying low-risk patients who may be suitable for early discharge or even non-admission. In the context of a recent UK audit, 4 SIGN guideline 5 and international consensus guideline on UGIH, 6 several publications have assessed scoring systems in an attempt to clarify their use by clinicians.
Scoring systems for UGIH
The most widely used score for UGIH is the Rockall score (Table 1). This was developed in 1996 7 to predict death after UGIH and used the data from an audit in four English Health regions. In addition to haemodynamic and laboratory data and features from the patient's history, calculation of the Rockall score requires endoscopy. An abbreviated ‘admission’ Rockall score (excluding the two endoscopic criteria) has been used in some centres, but this has never been fully validated. The Glasgow Blatchford Score (GBS) was developed in 2000 8 to predict a patient's risk of requiring intervention or death (Table 2). It does not include endoscopic findings and can be calculated shortly after presentation. The GBS has recently been shown to identify 16-22% of patients as being ‘low risk’ (GBS = 0; see Table 3) who could be safely managed as outpatients. 9
The Rockall Score
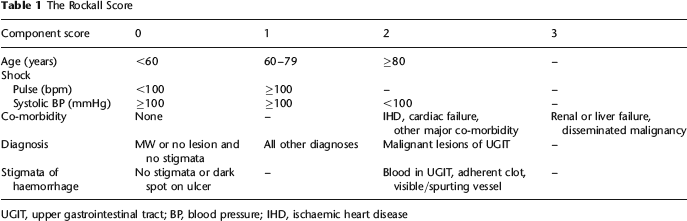
UGIT, upper gastrointestinal tract; BP, blood pressure; IHD, ischaemic heart disease
Glasgow Blatchford score (GBS)
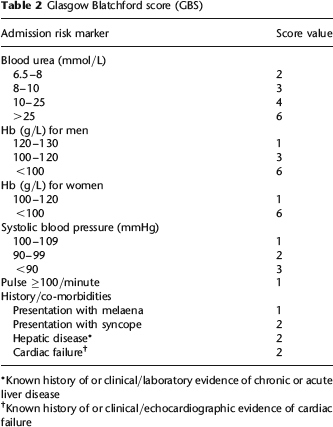
Known history of or clinical/laboratory evidence of chronic or acute liver disease
Known history of or clinical/echocardiographic evidence of cardiac failure
Glasgow Blatchford Score (GBS) ‘low-risk criteria’ (i.e. GBS = 0)

Other less commonly used endoscopically based scores include the Cipoletta, Longstreth, Hay, Imperiale and Baylor scores.10–14 In addition to the GBS, other non-endoscopic scores have been developed including the Cambridge score 15 and an American score based on an artificial neural network (ANN). 16 The Cambridge score requires 14 clinical and laboratory variables and identifies only 6% low-risk patients who may be suitable for outpatient management. Partly for these reasons it has not been externally validated or widely adopted. The ANN score requires 20 variables in addition to computer software for analysis, which makes it less attractive to busy clinicians. A summary of the main scores is shown in Table 4.
Summary of main risk scoring systems for UGIH

UGIH, upper gastrointestinal haemorrhage; ANN, artificial neural network
Clinical use of UGIH scores
Most patients presenting to hospital are admitted under general physicians or surgeons who may be unhappy discharging patients without re-course to specialty assessment and/or endoscopy. However, many Scottish and UK hospitals do not have an out-of-hours or weekend endoscopy service. A recent national UK audit of 6750 patients with UGIH has revealed that only 52% hospitals had an out-of-hours endoscopy service and only 50% patients received endoscopy within 24 hours of presentation. 4 Therefore many lower risk patients may stay in hospital longer than necessary, when outpatient management may be appropriate. Early and simple pre-endoscopy risk assessment has obvious advantages for use in A&E or acute receiving units.
While several scores are useful in identifying low-risk patients who may be suitable for early discharge, they appear less helpful in differentiating medium and higher risk patients who may require emergency endoscopy or high dependency/intensive care management. The variable availability of emergency endoscopy provision and high dependency and intensive care beds across Scotland and the UK, further complicate this issue. However the sensitivity of these scores is probably more important than the specificity, as the clinician does not want to mistakenly label a higher risk patient as ‘low-risk’ and possibly discharge them early. The most commonly used score in the UK is the Rockall score, although there is increasing use of the simple GBS on presentation, particularly to identify low-risk patients.
Recommendations from the SIGN guideline, the international consensus guideline and the UK national audit include early risk assessment of patients presenting with UGIH.5,6 The 2008 SIGN guideline suggested the use of the admission Rockall score, but was published before several recent papers directly comparing the GBS and admission Rockall scores, while the 2010 international guidelines recognized the recent favourable comparisons for the GBS. Use of the GBS for patients with UGIH has also been recently recommended by the NICE evaluated QIPP NHS evidence body (http://www.evidence.nhs.uk/aboutus/Pages/AboutQIPP).
Published comparisons of scores
One study assessed the three main endoscopy-based scores and found that the full Rockall was superior to the Cedars Sinai and Baylor scores, particularly for lower risk patients. 17 In this study, all scores were better at predicting mortality than re-bleeding. A recent large UK multicentre study reported the GBS to be superior to both the full and admission Rockall scores in prediction of need for intervention or death. 9 This study also confirmed the safety of avoiding admission in low-risk patients with a GBS of zero with no interventions or deaths in this group, whereas both of these endpoints were seen among patients identified as ‘low risk’ with an admission Rockall score of zero.
Other studies have recently compared the GBS and Rockall scores. A publication from Taiwan suggested that the GBS was superior to both the Rockall scores in predicting those at high risk for clinical intervention. 18 In this study, the GBS had a higher sensitivity than the admission Rockall score. A recent study from London also showed that the GBS was more sensitive and accurate than the admission Rockall score. 19 Studies from USA and Japan have shown a GBS of zero to have a 100% negative predictive value for re-bleeding or death, or need for intervention, respectively.20,21 Interestingly a multicentre North American study reported that a modified GBS (due to their non-recording of urea or syncope) was superior to the admission Rockall score in predicting high-risk endoscopic stigmata of bleeding or re-bleeding. 22 Recent data from Hong Kong have also shown the GBS to be superior to the admission Rockall score in predicting need for therapeutic endoscopy. 23 However the proportion of patients fulfilling the GBS low-risk criteria in this Chinese study was lower than the published UK figures, which may be due to differences in patient populations and healthcare delivery.
Conclusions
There is a growing body of evidence and consensus opinion to recommend the early use of risk stratification scores for patients presenting with UGIH. The GBS appears superior to the admission Rockall score for early non-endoscopic risk assessment and identifies low-risk patients in whom admission can be safely avoided. All scores seem to perform less well among patients at higher risk. Further studies are required to compare scoring systems in different populations and further clarify their role in clinical practice.