
Abstract
We present the case of a patient with an adenocarcinoma of the colon associated with an oncocytoma of the kidney. A left colonic cancer was diagnosed at colonoscopy and an incidental finding of a left renal mass was noted, with a staging computerized tomography scan. Following a left hemicolectomy and a left nephrectomy, the pathological report confirmed the presence of a colonic adenocarcinoma and revealed that the left renal mass was an oncocytoma. This case report reviews the management decisions associated with incidental renal masses as well as the treatment of synchronous neoplasia.
Case report
A 60-six-year-old gentleman presented with abdominal pain and an altered bowel habit. He reported pain in the hypogastric region, over the preceding four months. This was associated with a three-month history of increasing frequency of defaecation and intermittent fresh rectal bleeding. Although he had a good appetite and his weight remained steady, he reported that he had been feeling increasingly listless.
His past medical and surgical history included hypertension, diagnosed in 2002, and a pilonidal sinus, treated in 1962.
Physical examination was generally unremarkable. This gentleman was of a large stature and had a well-nourished appearance.
Investigations
Colonoscopy
A stricturing neoplasm was partially obstructing the lumen between the descending and sigmoid colon (Figure 1). Multiple biopsies were taken. A sessile 1 cm rectal polyp was also visualized and excised completely.
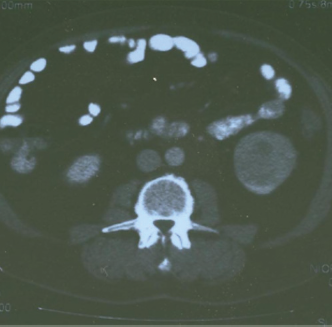
Computerized tomography scan – 62 mm mass at the lower pole of the left kidney suggestive of renal cancer. No liver or lung metastases were present
Pathology
Biopsies from the stricturing neoplasm were reported as invasive adenocarcinoma. The rectal polyp was found to contain an intramucosal adenocarcinoma that had been completely excised.
Imaging
Computerized tomography (CT) scan showed a left colonic mass suggestive of a cancer. An incidental 62 mm mass in the lower pole of the left kidney was also noted (Figure 2). No liver or lung metastases were present.

Colonoscopy – stricturing adenocarcinoma in the descending colon
Operative procedure
Two surgical teams, colorectal and urological, were involved in this gentleman's operation. Surgical access was obtained via a midline laparotomy incision. A standard left hemicolectomy with a side-to-side sutured anastomosis was performed. A left radical nephrectomy was also performed.
Histopathology
This showed a 34 mm moderately differentiated adenocarcinoma (Dukes’ B, pT4 NO) of the descending colon and a left renal oncocytoma measuring 55 mm.
Postoperative course
This gentleman's postoperative recovery was uneventful, and he was discharged home after eight days.
At three years after the procedure, the gentleman is well. Follow-up colonoscopy and CT scan do not show any signs of any local or distant recurrent disease.
Discussion
This is a case report regarding a 66-year-old gentleman who had successful open surgery for a left colonic cancer and a synchronous left renal oncocytoma. This is, to our knowledge, the only such report.
One cannot mention oncocytomas without crediting Zippel's first description back in 1942. 1 However, it was Klein and Valenci 2 who first carried out an observational study on this neoplasm. The incidence of renal oncocytoma varies from 3.2% to 7% of all primary renal tumours. 3 These masses are most often seen during the seventh decade of life, with a male to female preponderance of 1.6 to 1. 3 The diagnosis is usually incidental. Oncocytomas are found to be unilateral in 95% of cases, but are sometimes bilateral (5%), multifocal (6%) and metachronous (4%). 4
Many reports regard an oncocytoma as a distinct benign tumour. However, there is evidence to suggest that it has the ability to metastasize and cause death. 5 The very rare instances of renal oncocytoma metastases can be explained by a small population of oncocytomas sharing genetic and molecular features with clear cell renal carcinomas with a dominant eosinophilic component, or even with the eosinophilic variant of chromophobe renal cell carcinomas. 6 Furthermore, its ability to metastasize does not imply a more aggressive behaviour. 6
Although size is by no means diagnostic, it has been noted that with tumours larger than 3 cm there is an increased likelihood of more aggressive neoplasia. 7 Furthermore, a very large proportion of incidentally detected renal masses do actually prove to be malignant. So much so, that renal carcinoma accounts for 92% of incidentally discovered renal masses. Hence, it would make sense to regard any renal incidental mass as a low-stage renal carcinoma unless proven otherwise. 8
Modern imaging modalities have rewarded us with the ability to pick up incidental masses. However, it has become clear that both CT and magnetic resonance imaging (MRI) are unable to convincingly diagnose oncocytomas and to differentiate between oncocytoma and renal cell carcinoma. 9
Tissue sampling by core biopsy has been proposed as a further method of preoperatively diagnosing the pathology of incidental renal masses. A large review of reports from 1977 to 2006 by Volpe et al. in 2007, has concluded that this biopsy method is safe and with a 90% diagnostic yield. This group recommends that core biopsy should be considered, especially in the elderly and unfit. 10 However, other authors disagree and quote low rates of sensitivity and specificity, even when supplemented by CT. 11 The het-erogenous nature of the oncocytic neoplasm makes histological interpretation difficult and authors advise caution. 12
With some studies describing the benign nature of oncocytomas, some authors cast doubt on the need for surgical excision. They recommended a conservative or at least a non-radical approach towards this pathology. 3 However, other authors still advocate surgical excision as the standard treatment for this pathology. 13 This is due to the co-existence with renal cell cancer presenting at rates between 10% and 32%.4,14 Since then, a further report has shown a hepatic metastasis from a focal area of chromophobe renal cell carcinoma within an oncocytoma. 15 This example of a ‘wolf in sheep's clothing’ has raised concern. However, it has also been reported that two cases showing suspicious high mitotic activity and atypical mitotic figures associated with renal cell carcinoma and cystic disease, were disease free at 42 and 54 months follow-up. 3 With the current evidence it is unlikely that patients will avoid surgery until other forms of renal neoplasia are ruled out preoperatively.
The incidence of synchronous renal and colorectal neoplasia varies from study to study. An Italian study reported an incidence of 0.4%, and the authors simply recommend an increased level of vigilance. 16 On the other hand, a group from Israel, who reported an incidence of 4.85%, has gone as far as recommending the assessment of colon cancer patients with urine cytology and imaging techniques. 17
The primary treatment of synchronous colorectal and renal carcinoma is surgical. Our patient had a successful open repair by a colorectal and urological team. Although open surgery is the standard procedure, it has also been shown that these operations can be safely performed laparoscopically.18,19 Ng et al. have reported good surgical and oncological outcomes for their five cases, with a median operating time of 420 minutes and a median blood loss of 1 litre.
In conclusion, this is the first report of a case of a synchronous colonic adenocarcinoma and renal oncocytoma. In view of the ongoing debate of preoperative CT and MRI scans and core biopsy histology to differentiate between oncocytomas and renal cancer, we recommend radical surgical resection of both the colonic and renal neoplasm without prior renal biopsy. Adjuvant treatment is then administered depending on the results of staging and the general condition of the patient.
The authors declare that they have no competing interests.