
Abstract
A case report of a patient presenting with painless arm swelling, which provides diagnostic challenge and interesting imaging on the conditions of syringomyelia and neuropathic osteoarthropathy, conditions with distinguishing clinical features and disabling consequences if misdiagnosed.
A 73-year-old lady was referred by the community physiotherapist with weakness and gross swelling of the right arm. There was no history of trauma but she did complain of 12 months of neck pain and arm weakness, recently becoming worse on the right. Accidental cuts and burns were also noted, without associated pain.
The latter were explained when she disclosed a diagnosis of syringomyelia 20 years earlier; intervention had not been appropriate and she had been lost to follow up. Her other health problems included hypertension, a transient ischaemic attack and asthma.
Examination demonstrated pitting oedema of both ankles but cardio-respiratory systems were otherwise unremarkable. Her right arm was grossly swollen and intrinsic muscles of the hands appeared wasted; range of movement of the right hand and wrist were good, but reduced at the shoulder in all directions. Cranial nerves and higher cortical function were normal; tone and reflexes were increased in the lower limbs, with extensor plantar responses; and power, tone and reflexes were diminished in the upper limbs, particularly distally. Dorsal column sensation was intact, but pinprick and temperature sensation were reduced over C2 to T5 dermatomes.
Investigation of the arm swelling revealed a raised d-dimer and inflammatory markers, normal leukocyte count and microcytic anaemia. Our differential diagnoses included venous thrombosis or lymphatic obstruction of the right arm, but Doppler sonography excluded right arm venous thrombosis.
She became tachycardic and hypotensive and a computerized tomography pulmonary angiogram was arranged; this ruled out pulmonary embolus but suggested trauma to the right shoulder, although she still denied pain or injury. Imaging (Figure 1) confirmed a comminuted fracture of the proximal humerus, calcification in the rotator cuff and deltoid and an effusion. The unifying diagnosis of neuropathic osteoarthropathy (Charcot's joint) secondary to synringomyelia became apparent, magnetic resonance imaging confirming syrinx from C2 to C6 level (Figure 2). No active management was instigated, but she was followed up by neurology and physiotherapy departments as an outpatient.

Three-dimensional reconstruction of computerized tomography images demonstrate neuropathic osteoarthropathy of the right shoulder
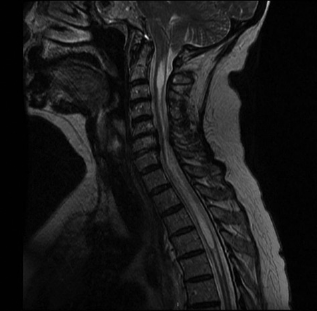
Magnetic resonance imaging of the cervical spine demonstrates syringomyelia C2-C6
Cerebrospinal fluid (CSF) is normally contained within the ependyma of the central canal; obstructed CSF outflow due to Chiari malformation, trauma, haemorrhage, radiation, infection or intramedullary tumours can cause CSF to dissect into white matter, forming a syrinx (cyst). Syringomyelia interrupts the spinothalamic fibers decussating near the centre of the cord, causing loss of pain and temperature sensation; more distal dorsal columns are generally spared. Distribution can be either or both arms, or a shawl pattern; dysaesthesia of the neck and shoulders and radiculopathy can also occur.
Motor signs show a distinctive pattern of upper-limb lower-motor neuron weakness and hyporeflexia, that progress proximally as ventral nerve roots are compressed, with lower-limb upper-motor neuron signs if a syrinx is large enough to affect corticospinal tracts. Less commonly, bladder, bowel and sexual dysfunction are seen, and Horner's syndrome may also occur if sympathetic nerve fibres are disrupted.
The hypothesized pathophysiology of neuropathic osteoarthropathy is sensory impairment leading to (unnoticed) repetitive trauma and inflammatory bone resorption, 1 along with vasomotor dysregulation causing hyperaemia and osteoclast activation, 2 thus progressive bony destruction, deformity and loss of function.
The commonest causes are diabetic and alcoholic neuropathy, although cerebral palsy, spinal cord trauma or syringomyelia, infections (leprosy, syphilis) and even nerve damage from intra-articular steroids can all result in neuropathic osteoarthropathy. Figure 1 demonstrates the radiographic features – a disorganized joint with bone destruction and dislocation.
Acute management involves immobilization and bisphosphonates; longer-term includes orthotics, physiotherapy and education, alongside measures to prevent further sensory loss. Surgery has a role in malaligned, unstable or non-reducible joints, 3 the failure rate of arthro-plasty and arthrodesis, however, is high.
Conclusion
A high index of suspicion aids early diagnosis of syringomyelia and neuropathic osteoarthropathy, if disabling consequences are to be avoided. Any patient whose deformity seems disproportional to their pain should have neuropathy excluded through neurological assessment of sensation and imaging.
Footnotes
Acknowledgement
Many thanks to Dr R Madhok for his guidance. Patient ‘Consent to disclose’ is obtained. There is no conflict of interest, financial or commercial interest and the author accepts responsibility for the content of the manuscript as true and original work.