
Abstract
Our aim was to explore the clinical application value of high-intensity focused ultrasound (HIFU) therapy for tubal pregnancy. Forty hospitalized patients with tubal pregnancies (28 cases of non-ruptured tubal pregnancy and 12 cases of ruptured tubal pregnancy) were selected to receive HIFU therapy. Serum human chorionic gonadotropin (β-HCG) concentrations were compared before and after treatment. Serum β-HCG was measured weekly and patients received observation only if the concentration decreased by 15% or more, compared with the previous value. Patients were given supplement HIFU therapy if the decrease in the serum β-HCG was <15% within two weeks. Ultrasound was used to detect the volume changes in the ectopic lesions before and after treatment, and changes in vital signs and complications were recorded. Contrast-enhanced ultrasonography was used to assess fallopian tube patency after treatment. HIFU treatment was successful in 33 of the 40 patients (82%). Seven patients failed HIFU treatment and received surgical therapy (18%). Before and after treatment, serum β-HCG concentrations and lesion volume were significantly different (P < 0.05, P < 0.01, respectively). Post-treatment tubal contrast-enhanced ultrasonography showed tubal patency on the affected side in 21 cases (64%) at six months and in 27 cases (82%) at 12 months. In conclusion, HIFU is safe and effective, and can be a treatment option for tubal pregnancy.
Introduction
Ectopic pregnancy refers to implantation and development of a fertilized ovum outside of the uterine cavity,1,2 of which tubal pregnancy is the most common type. 3 It is a common gynaecological cause of an acute abdomen in adult females and can be life threatening. Ultrasound imaging techniques including two-dimensional greyscale ultrasound, colour Doppler ultrasound and power Doppler are important modalities for the diagnosis of ectopic pregnancy.4,5
In recent years, rapidly developing ultrasound techniques have played an important role in the imaging diagnosis of diseases as well as in the treatment of many conditions. 6 High-intensity focused ultrasound (HIFU) is a non-invasive ablation technique that uses an extracorporeal high-energy acoustic beam focused on the designated target tissues in the body to cause ablation. It can cause coagulation necrosis of tissue through thermal effects, cavitation effects and sonochemical effects, and it usually will not injure the surrounding tissues.7,8 Currently, HIFU has been widely used in clinical treatment of many diseases and in related experimental studies.9-11 HIFU ablation provides another treatment option for solid, benign and malignant tumours of abdominal and pelvic organs, and it plays a role in extending survival and alleviating pain in patients with end-stage cancer. There has been a report on the successful application of HIFU for the treatment of uterine fibroids. 12
Common methods for treating ectopic pregnancy are surgical and conservative treatment,13-15 but both may cause different degrees of damages to the body. HIFU is known as a green therapy because it is a safe, non-invasive, accurate and effective treatment. This study explored the therapeutic effects of HIFU for the treatment of ectopic pregnancy, which may provide a new non-invasive method for the treatment of ectopic pregnancy.
Material and methods
Patients
Forty patients with confirmed diagnosis of ectopic pregnancy treated at the Department of Gynecology and Obstetrics of our hospital from August 2006 to July 2008 were included. The average patient age was 25 + 5 years (range, 20-32 years). Ectopic lesions were found by both transvaginal and transabdominal ultrasonography. Serum human chorionic gonadotropin (β-HCG) concentrations were increased with values ranging from 580 to 1978 mlU/mL (average, 880 mlU/mL). The lesion volume was calculated using the formula: volume = (anteroposterior diameter x transverse diameter x longitudinal diameter x π)/6 cm3. Inclusion criteria for HIFU therapy were: (1) site of the tubal pregnancy was identified on transabdominal ultrasound, and the diameter of the gestational sac was less than 3 cm; (2) the estimated volume of the liquid in the rectal fossa was less than 100 mL; (3) there was no fetal heart beat; and (4) no maternal heart, liver, kidney and blood disorders occurred. Exclusion criteria were: (1) intralesional bleeding existed; (2) the patients having severe maternal liver or kidney damage; and (3) β-HCG was over 2000 mlU/mL.
Equipment
The HIFUNIT 9001 tumor ablation system (Shanghai Aishen Technology, Shanghai, China) was used. This device has six therapeutic transducers and can focus the ultrasound beam through two times focalization. The frequency of the ultrasound wave was 1.0 MHz, and the focal intensity was 0-3000 W/cm2. The focal length was 13.42 cm and the dimensions of the focal region were 3 mmx3 mmx8 mm. Routine ultrasonography was performed with an Acuson Sequioa 512 (Siemens, Erlangen, Germany) equipment and a 4V2 abdominal convex ultrasound probe (Siemens). Contrast-enhanced ultrasonography was performed with an EV8C-4 transvaginal probe (Siemens). The ultrasound contrast agent used was SonoVue (Bracco, Milan, Italy), which was mixed with 5 mL normal saline to produce a microbubble suspension before use.
HIFU therapy
The patients received pretreatment transabdominal ultrasonography to determine the lesion site, which was marked on the body surface. An amount of ultrasound coupling gel, close to the size of the HIFU device head, was applied onto the therapeutic area and full coupling between the therapeutic head and the therapeutic area was assured. Intraoperative parameters were as follows: each sonication lasted 0.15-0.2 seconds, and the interval between two sonications was 0.3-0.4 seconds. There were four to six sonications and the number of transducers was 3-4. The power utilized was 60-80%. Intraoperative monitoring was performed with the Acuson Sequioa 512 machine.
Contrast-enhanced ultrasonography of the oviduct
Re-canalization of the fallopian tube on the affected side was examined by contrast-enhanced ultrasonography six months and one year after treatment. Patients received contrast-enhanced ultrasonography 3-7 days after menstruation. The bladder was moderately full and the patient was in the lithotomy position. After disinfection and draping, the cervix was exposed and fixed, and a uterine double-lumen tube was inserted. One millilitre of diluted SonoVue ultrasound contrast agent was injected, followed by an injection of 20 mL normal saline. The pressure during injection was felt and determined by the same doctor. The following criteria were used to determine patency of the tube: (1) the fallopian tube was considered unobstructed if the injection met no significant resistance; abdominal pain was not apparent; microbubbles flowed rapidly towards the fallopian tube and could be seen throughout the entire fallopian tube with ‘jet sign’ seen on the umbrella side; fluid accumulation or increased fluid accumulation could be seen in the rectal fossa 15 minutes after injection of the contrast agent (Figure 1a).
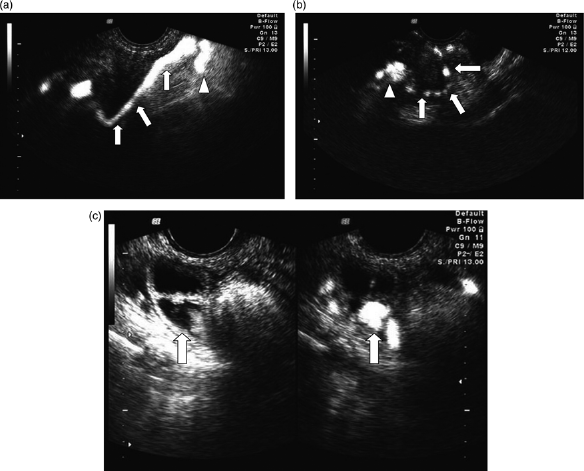
Ultrasound images of lesions before and after treatment. (a) Tubal patency. Microbubbles flowed towards the fallopian tube (arrows) rapidly. Hyperechoic air bubbles could be seen throughout the entire fallopian tube, and the ‘jet sign’ is seen on the umbrella side (arrowhead). (b) Partial obstruction. Microbubbles flowed slowly in the lumen, and the fallopian tube (arrows) exhibits thin broken-line-like strong echoes. A small amount of air bubbles overflow from the umbrella end (arrowhead), and some reflective circular strong echoes are seen around the ovary. A small amount of fluid is present in the rectal fossa. (c) Distal tubal obstruction. Microbubbles flowed slowly in the fallopian tube or gathered together, and fluid accumulation (arrows) occurred. No image of the distal end is apparent and reflux to the uterus occurred. There was no obvious fluid accumulation in the rectal fossa. Left: greyscale ultrasonography image; Right: contrast-enhanced ultrasonography image
(2) The fallopian tube was considered unobstructed, but the patency was poor if the injection met some resistance (the fluid could be injected slowly with added pressure); the patient experienced slight abdominal pain during injection; microbubbles flowed slowly in the lumen, and the fallopian tube showed thin broken-line-like strong echoes; a small amount of microbubbles overflowed from the umbrella end, and some hyperechoes were seen around the ovary; a small amount of fluid was seen in the rectal fossa (Figure 1b).
(3) The fallopian tube was considered obstructed if the injection met considerable resistance. When pressure was added, the patient experienced obvious abdominal pain; the microbubbles flashed, and flowed slowly in the fallopian tube, or gathered at a certain segment. The distal end of the fallopian tube was not visualized and reflux sometimes occurred. There was no obvious fluid accumulation in the rectal fossa (Figure 1c).
Efficacy assessment
HCG levels were observed before and after HIFU therapy. The size and echogenicity of lesion were evaluated by greyscale ultrasonography. Internal blood flow of the lesion was measured before and after HIFU therapy on colour Doppler ultrasonography.
The therapeutic effects were divided into effective and ineffective. The criteria for effective treatment were serum β-HCG level decreased by 15% or more, seven days after therapy as compared with the initial value, and the serum β-HCG level was <10 mlU/L at one month after treatment. The criteria for ineffective treatment were serum β-HCG level decreased by <15% or increased seven days after therapy as compared with the initial value, the patient received surgical treatment, the fluid volume in the rectal fossa increased significantly within one month, or a fetal heart beat appeared. 1
Statistical analysis
SPSS version 11.5 statistical software (SPSS Inc, Chicago, IL, USA) was used. The measurement data were shown as mean + standard deviation. The t-test was used to analyse changes in the various parameters. A P value <0.05 was considered to indicate a statistically significant difference and a P value <0.01 was considered to indicate a greatly significant difference.
Results
The maximum volume of the ectopic lesions was 27.4 cm3, the minimum volume was 15.2 cm3 and the average volume was 26.2 cm3, as measured on transabdominal ultrasonography.
Serum β-HCG changes
Serum β-HCG changes are presented in Figure 2. One week after the first HIFU treatment, the serum β-HCG level decreased by >15% compared with the initial value in 14 of 40 patients. Serum β-HCG level decreased by > 15% in 11 patients compared with the previous values at two weeks after treatment. The serum β-HCG level decreased by >15% in 15 patients compared with the previous values after two weeks, and those patients received a second HIFU treatment. There were seven patients whose serum β-HCG level decreased by > 15% compared with the previous values at weeks 3 and 4. One patient received three HIFU treatments and her serum β-HCG level decreased by > 15%. The serum β-HCG level decreased to <10 mlU/L in 33 patients (82%) within four weeks. A total of seven patients failed HIFU treatment (18%). Among the patients who failed HIFU treatment, a fetal heartbeat appeared in the gestational sac in four patients after one or three HIFU treatments, and serum β-HCG level was increased compared with the initial value. As a result, those patients were treated with other methods. The serum β-HCG level was increased in three patients compared with the initial values after one or three HIFU treatments, and fluid accumulation in the rectal fossa increased significantly, suggesting that the gestational sac was ruptured. Therefore, surgical treatment was adopted for those patients.
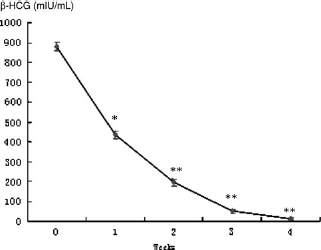
Mean concentrations of post-treatment serum human chorionic gonadotropin β-HCG. Serum β-HCG level was checked weekly, and was compared with the initial value. *P < 0.05, **P < 0.01
Ultrasound imaging of the lesions and volume changes
After HIFU treatment, local high temperature caused coagulation necrosis of the internal tissue of the gestational sac and the blood vessels in the lesions were obstructed. Before treatment, scattered thin blood flow signals could be observed in the lesions in 25 patients. After treatment, no blood flow signals were observed in the lesions of 20 patients, but blood signals were more abundant on the edge of the lesions.
After treatment, echoes were enhanced or slightly enhanced in the lesions in 24 patients (21 cases of the non-ruptured type, and 3 cases of the ruptured type in which the echoes of the surrounding tissues were slightly enhanced; Figure 3). The borders of the lesions were clearer with uneven internal echoes. Subsequently, the lesion size changed gradually.

Ultrasound images of lesions before and after treatment. (a) Two-dimensional ultrasound image of an ectopic pregnancy before treatment. The echo of the lesion was diminished, and a theca luteinized cyst was present. (b) Fifteen days after high-intensity focused ultrasound treatment, the lesion echo was slightly enhanced. The lesion exhibited a clear boundary and reduced size, and the theca luteinized cyst was not present
The lesion size was significantly decreased in 19 patients after 15 days, as compared with the initial value (P < 0.05). At day 30, the lesion size was significantly decreased in 26 patients (P < 0.01). Lesions were clearly visualized or had disappeared in 31 patients after 45 days. In two cases, post-treatment lesion sizes were not significantly different from the initial values (P > 0.05). At six-month follow-up, a small mass was revealed by transvaginal ultrasound at the previous therapeutic site in two patients, but no mass was found by transvaginal ultrasound at 12 months. Seven patients were not included in this analysis because they received surgery or another treatment method. Comparisons between the mean post-treatment lesion volume and the initial values are shown in Figure 4.

Changes in post-treatment ectopic lesion volume. The ectopic lesion volume was checked every 15 days and was compared with the initial value. *P < 0.05, **P < 0.01
Post-treatment follow-up results
We performed contrast-enhanced ultrasonography of the fallopian tube in 33 patients with tubal pregnancies, six months after HIFU treatment. Tubal patency of the affected fallopian tube was observed in 21 patients (64%). The fallopian tube showed some blockage in nine patients (27%), of which four patients had experienced previously. The fallopian tube was obstructed in three patients (9%). After 12 months, tubal patency of the affected fallopian tube was observed in 27 patients (82%), the fallopian tube showed poor patency in five patients (15%) and one patient experienced fallopian tube obstruction due to adhesion (3%) (Table 1).
Results of high-intensity focused ultrasound therapy
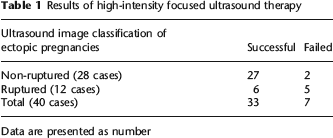
Data are presented as number
Discussion
A common conservative treatment is to terminate the pregnancy using mifepristone in combination with methotrexate. However, their side-effects include nausea, vomiting and white blood cell count decrease. Therefore, the discovery of a safe, effective, non-invasive, painless treatment has received more and more attention. 16 Currently, HIFU has been applied in multidisciplinary cancer treatment, in which the mechanism of tumour inactivation is to cause cellular protein denaturation through instantaneous high temperature in target tissues, resulting in coagulation necrosis and subsequent organization, absorption or fibrosis.17,18
Serum β-HCG concentrations after one and three treatments were significantly different from the initial values, suggesting that HIFU treatment can inactivate embryo chorionic villi in patients with an ectopic pregnancy, thus terminating the pregnancy. Changes in the ectopic lesion size and further in serum β-HCG levels, indicated that if HIFU treatment was effective, serum β-HCG levels would decrease and lesion volume would be reduced, and there was a linear relationship between them. However, lesion size reduction lags behind β-HCG decrease.
The therapeutic effects of HIFU treatment were considered better for non-ruptured ectopic pregnancies than for ruptured, which might be related to the internal tissue structure of the lesion. Non-ruptured ectopic lesions mainly consist of solid components, while ruptured ectopic lesions consist of solid and liquid constituents. Therefore, the former may have a higher capacity for thermal absorption than the latter. Similarly, post-treatment echo intensity was increased in non-ruptured lesions as compared with ruptured lesions, and the internal blood flow signals were significantly reduced in ruptured lesions, indicating that changes in ultrasound images may indirectly reflect the therapeutic effect. Additionally, patients who failed HIFU treatment (7 cases) had ruptured ectopic pregnancies and the reason for treatment failure may be related to the poor local thermal effects of HIFU treatment in larger lesions containing more internal liquid areas. Therefore, we believe that non-ruptured ectopic pregnancy is the primary indication for HIFU treatment.
Some patients experienced pulse, blood pressure and respiratory rate changes during treatment, which were considered to be related to emotional stress caused by a lack of understanding of the treatment. The patients recovered rapidly after the treatment was stopped.
Based on the post-treatment follow-up data, we believe that the embryonic tissues may go through a series of pathological changes after HIFU treatment; including liquefaction, necrosis and ultimately fibrosis, and adhesions may occur in the surrounding tissues due to the ‘ultrasonic welding’ phenomenon. However, whether or not fallopian tube adhesions and obstruction will occur in patients after HIFU treatment is of great importance for patients who desire fertility, especially for patients in whom the contralateral fallopian tube is absent or obstructed. We carried out follow-up examinations in 33 patients who received HIFU therapy and the results indicated that 94% of the masses were completely absorbed at six months, and all the masses were completely absorbed after one year. Contrast-enhanced ultrasonography showed that tubal patency of the affected tube at one year was significantly better than at six months. Complete mass absorption does not equal complete tubal patency, and complete fallopian tube repair lags behind mass absorption. Recovery of tubal patency also depends on the quality of the fallopian tube itself. However, the results of the contrast-enhanced ultrasonography at one year, showing good tubal patency after HIFU therapy, indicate that tubal morphology and function is not irreversibly affected by HIFU treatment.
HIFU therapy has obvious advantages compared with traditional conservative treatment for tubal ectopic pregnancies. It has been shown that HIFU treatment reaches an effective therapeutic temperature within a short time, thus inactivating the gestational sac without injuring the surrounding tissues, which might prevent tubal adhesions.19,20 The results of this study are consistent with these findings, further suggesting that HIFU therapy will not cause more complications or aggravate disease conditions when it is used for the treatment of tubal ectopic pregnancy.
In conclusion, HIFU can be used for the treatment of ectopic pregnancy. Compared with common traditional treatments, it is safe, non-invasive, less painful and practical with good repeatability and has no significant side-effects. However, longterm post-treatment follow-up and large sample studies are still needed.