
Abstract
Cystic adventitial disease (CAD) is rare. The popliteal artery is the most commonly affected artery. Patients with CAD are usually young and present with ischaemic lower limb symptoms. We report a case of a 39-year-old male patient with popliteal CAD. The affected segment was resected and repaired with an interposition vein graft. In conclusion, we highlight the importance of correct diagnosis and outline the different management strategies.
Introduction
Cystic adventitial disease (CAD) is rare, with the average vascular surgeon seeing only a few cases in their career. CAD is important to detect, as the luminal narrowing caused by the cystic lesion in the arterial adventitia can rapidly progress to disabling claudication or critical limb ischaemia. We report a case of a patient with popliteal CAD and highlight the importance of correct diagnosis and outline the different management strategies.
Case presentation
A 39-year-old man who was a keen amateur footballer presented to a sports injury clinic with a sudden onset deep right calf pain brought on by exercise. This was associated with altered sensation of the toes. Symptoms resolved with rest. His past medical history included adrenal cortical insufficiency for which he took steroid replacement. He did not have any risk factors for peripheral arterial disease. A diagnosis of possible chronic compartment syndrome was made. After three months, despite rest, his symptoms worsened and he was referred to orthopaedics for further assessment and possible fasciotomy. On examination the right femoral pulse was palpable but nothing below this. There was right foot pallor with elevation. A vascular pathology was suspected. He was then referred to the vascular department which identified a good history for intermittent claudication and confirmed the above clinical findings. A combined magnetic resonance imaging (MRI) and MR angiogram was performed, and demonstrated a cyst in the wall of the popliteal artery together with a complete occlusion of the affected vessel (Figures 1 and 2). Popliteal CAD was diagnosed. The affected segment was resected and repaired with an interposition vein graft via a posterior approach. The patient was discharged mobilizing without difficulty and will be reviewed in the outpatient clinic.

Magnetic resonance image of right popliteal cystic adventitial disease (arrow)
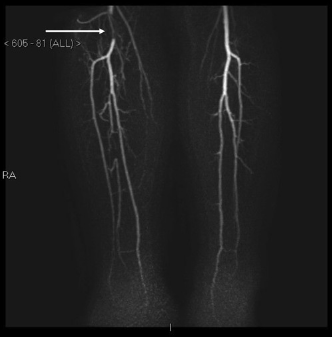
Magnetic resonance angiogram showing the right popliteal occlusion (arrow) caused by the cystic adventitial disease
Discussion
CAD is rare, with only 300 cases reported in the literature.1,2 CAD is characterized by unilocular or multilocular mucinous gelatinous cysts in the adventitial layer of the vessel wall. The popliteal artery is the most commonly affected artery (85% of cases). CAD is not associated with a systemic disorder and there is no report of a second vessel affected in the same patient. CAD is typically a condition affecting young men (age 40-50 years, M:F, 5:1).
The exact aetiology remains unclear. Several theories have been proposed which include developmental, synovial, trauma and systemic.3,4 The systemic and trauma theories have little supporting evidence.
Diagnosis is easily missed or delayed for the unwary clinician as the patients are commonly young, active and without risk factors for peripheral arterial disease. Early recognition is important as CAD is often rapidly progressive and can lead to critical limb ischaemia. 5 Patients often present with acute onset of claudication symptoms. This can be associated with neurological symptoms likely due to the pressure effect of the cyst on the lateral popliteal nerve. It is important to differentiate between the more common conditions in athletes such as muscular origin, chronic compartment syndrome, stress fractures or medial tibial stress syndrome as each have different treatments. An alternative vascular cause of exertional leg pain in young patients is popliteal artery entrapment syndrome (PAES) (aberrant relationship between popliteal artery and gastrocnemius muscle). Differentiation between CAD and PAES is made on imaging.
Clinical findings are unreliable. Popliteal and pedal pulses are often present and a popliteal lump is rarely palpable. Ishikawa et al. 6 reported the disappearance of foot pulses on knee flexion but this has also been described in normal cases. Therefore a diagnosis of CAD should be considered in all young patients with ischaemic symptoms.
Owing to the rarity of the condition, little is known about the non-invasive imaging modality of choice. The choice lies between arterial duplex, computed tomography and MRI. Combined MRI and MR angiogram appears to be the more favourable imaging modality. 7 This can evaluate the extent of the cystic disease and extent of arterial stenosis, therefore providing the most accurate guidance for surgical planning. Angiography appearances often show a characteristic smooth tapering stenosis or smooth hourglass appearance of the affected artery. But appearances may be normal or show complete occlusion, resulting in missed or incorrect diagnoses. 8
Unlike claudication caused by atherosclerosis, patients with CAD require intervention as spontaneous resolution is extremely rare. The management options can be divided into CAD with a patent popliteal artery and CAD with an occluded popliteal artery. 9
Management of CAD with patent popliteal artery includes percutaneous drainage or open excision of the adventitial cyst. Percutanous drainage is temporary and is not regarded as definitive treatment. Excision of the adventitial cyst preserves the artery and avoids the complications of the interposition graft. Subsequent aneurysm formation has not been reported. If recurrence does occur, this is probably related to failure to recognize multiple cysts at the initial operation.
The majority of cases of CAD with popliteal artery occlusion have been treated with excision of the affected segment and reconstruction with an interposition vein graft.
Percutaneous angioplasty has been described in the literature. But this technique is not effective, as the stenosis recurs due to the compliant affected artery. 10
Conclusion
In summary, the diagnosis of CAD should be considered in all young adults presenting with ischaemic symptoms. Clinical signs are often absent. Early diagnosis is important to prevent progression to disabling claudication or in the worst case critical limb ischaemia.