
Abstract
A 77-year-old woman presented with subacute respiratory symptoms which were demonstrated to be due to nocardiosis. After initial improvement with antimicrobial therapy, new symptoms appeared, consisting of persistent vomits, abdominal pain and hypotension, which led to the diagnosis of Addison's disease.
Keywords
Introduction
Nocardiosis is an infection caused by bacteria of the genus Nocardia. Pneumonia is the most common clinical presentation, but disseminated disease and a variety of localized manifestations, such as brain abscess or cellulitis, are not rare with the condition. 1
We report a rare case of nocardiosis, caused by Nocardia farcinica, which was complicated with the development of Addison's disease.
Case report
A 77-year-old woman presented with a one-month history of intermittent non-oppressive diffuse chest pain, nonproductive cough, low-grade fever and loss of appetite. Her past medical record was remarkable because of longstanding hypothyroidism which had developed after thy-roidectomy, carried out for the treatment of multinodular goiter. Axillary temperature was 38°C, a grade 3 systolic murmur was heard over the aortic area and scattered rales were present in both lung field; otherwise physical examination was normal. Blood analysis showed white blood cell count 14,400 per mm3, with left deviation, haemoglobin 8.6 g/dL, mean corpuscular volume 76 fL, erythrocyte sedimentation rate 120 mm in the first hour, ferritin 1221 ng/mL, iron 11 μg/dL and albumin 1.8 g/dL, while all other results were normal. Chest radiographs revealed a mild pleural effusion. A computed tomography (CT) scan of the chest disclosed tenuous patchy infiltrates in both lung fields (Figure 1), a mild pericardial effusion and a minimal pleural effusion. An electrocardiogram, an echocardiogram, an abdominal ultrasound and a magnetic resonance imaging of the head were normal. Three sputum cultures grew N. farcinica, while blood and urine cultures were negative. Serological tests, including those of acute cytomegalovirus infection, were also negative. Treatment was instituted with sulphamethoxazol-trimethoprim (75 mg per kg per day in 3 divided doses and 15 mg per kg per day in 3 divided doses, respectively), with disappearance of fever, and resolution of lung infiltrates, and pericardial and pleural effusions. Nevertheless, nausea and vomiting, abdominal pain and hypotension appeared, and vomits rapidly became persistent and uncontrollable. New blood analysis revealed sodium 112 mEq/L and potassium 5.4 mEq/L. Sixty minutes after 250 μg of intravenous cosyntropin, cortisol was 9.3 μg/dL. Basal adrenocorticotropic hormone (ACTH) level was 64 pg/mL. Adrenal antibodies were negative. A CT scan of the abdomen showed a contrast-enhanced swelling of both adrenal glands. Upper and lower gastrointestinal endoscopies were unrevealing. Treatment was instituted with hydrocortisone (20 mg in the morning and 10 mg in the evening) and fludrocortisone (0.1 mg per day), with a complete resolution of symptoms and normalization of all blood analyses abnormalities. Three months later, while on treatment with hydrocortisone and fludrocortisone, the patient was asymptomatic.
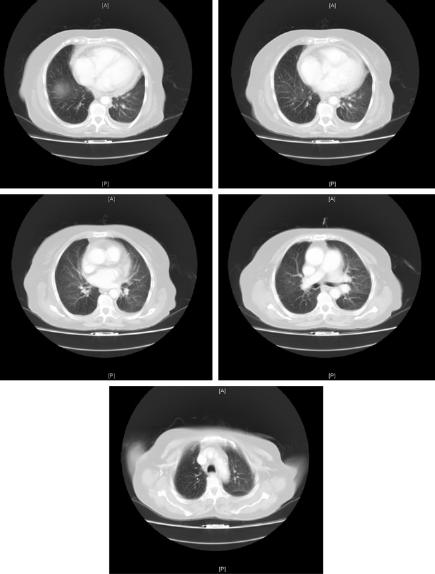
Computed tomography (CT) scan of the chest of the patient, showing tenuous patchy infiltrates in both lung fields, a mild pericardial effusion and a minimal pleural effusion
Discussion
Nocardia asteroides is the most frequent aetiological agent of nocardiosis, but several other species may be involved. N. farcinica is an uncommon cause of the disease, but the organism is more virulent than most other species of Nocardia, and is generally responsible of disseminated forms of the infection. 2
Nocardiosis occurs worldwide and affects persons of all ages, but is much more prevalent in patients with deficient cell-mediated immunity. Infection is thought to occur after inhalation of the bacteria. The most typical clinical presentation is subacute pneumonia, which may be followed by direct or haematogenous dissemination. In these ways, virtually any tissue of the organism can be affected by the disease. Abscess formation can occur, and sometimes fistulization and discharge of pus takes place. Cutaneous inoculation, usually followed by cellulitis and lymphadenitis, can also occur. 3
Addison's disease primary adrenocortical deficiency is an uncommon disease that occurs at any age and affects both sexes equally. The condition results from destruction of the adrenals, and clinically is characterized by a variety of symptoms. These generally include weakness, anorexia, nausea and vomiting, weight loss, cutaneous and mucosal hyperpigmentation, and hypotension, but depending on the duration and degree of adrenal hypofunction, the manifestations may vary substantially, from isolated mild chronic fatigue to fulminating shock. Diagnosis is made by demonstrating an impaired response of the adrenals to ACTH stimulation, associated with an elevated plasma ACTH level and treatment consists of replacement of both glucocorticoid and mineralocorticoid hormones. 4
Decades ago, Addison's disease was most commonly caused by tuberculosis and other granulomatous infectious diseases, like histoplasmosis, coccidioidomycosis and cryptococosis. Nowadays, some cases of Addison's disease are still produced by those infections, or other conditions such as sarcoidosis, adrenoleukodystrophy, bilateral adrenal haemorrhage, tumour invasion, cytomegalovirus infection, but most cases are idiopathic, with an autoimmune mechanism probably involved.5-7
In a review of the literature by means of a Medline search using ‘Nocard* AND (Addison OR Addison's OR adrenal)’ as search strategy keywords, we have found only one more report of Addison's disease associated to nocardiosis, which occurred in an HIV-infected patient and was caused by N. asteroides. 8
Conclusion
Rare complications of nocardiosis can take place;
We present a case of nocardiosis complicated with Addison's disease.