
Abstract
Beta-blockers are recommended as first-line symptomatic treatment for stable angina. However, their impact on mortality outside the context of myocardial infarction is unknown. We performed a meta-analysis of all randomized trials of beta-blockers in stable angina. Medical databases and cardiology journals were searched for relevant randomized clinical trials. The primary outcome was cardiovascular mortality, separately considering trials of beta-blockers versus placebo and beta-blockers versus other antianginals. We conducted a subgroup analysis on cardioselective versus non-cardioselective beta-blockers and calcium channel antagonists versus nitrates. We calculated odds ratios (ORs) and confidence intervals (CIs) using Peto's method. We found no statistically significant evidence that beta-blockers impact on mortality when compared with placebo (OR, 0.42; CI, 0.15–1.21) or other antianginals (OR, 0.98; CI, 0.86–1.10), or all others (OR, 0.97; CI, 0.86–1.09). There was a trend for cardioselective beta-blockers to have a greater improvement in mortality when compared with placebo and to have greater impact than non-calcium channel antagonists. Beta-blockers do not have statistically significant impact on mortality versus placebo or versus other active comparators. The findings exclude a benefit of 15% or greater and a hazard of 10% or greater. The impact of cardioselectivity requires further study.
Introduction
Beta-blockers are recommended in guidelines as one of the key classes of treatment for symptomatic relief of stable angina. 1 By inhibiting beta receptors and causing a reduction in inotropic state and sinus rate, they reduce the oxygen demand and relieve the symptoms of angina. 2 Cardioselective beta-blockers have greater affinity 3 for the beta-1 receptors found mainly in cardiac tissue. 4 Meta-analyses have shown that beta-blockers remain the first-line drugs for the long-term prevention of chest pain resulting from coronary heart disease.5–7
Whether beta-blockers have an impact on the mortality of patients with stable angina remains unclear. A meta-analysis published in 1999 6 found no significant differences with regard to mortality when beta-blockers were compared with calcium channel blockers, but, surprisingly, no meta-analysis has been published in the last decade comparing beta-blockers with either placebo or other antianginals.
Beta-blockers are of prognostic benefit following myocardial infarction (MI),8,9 and a large observational nonrandomized study found that beta-blockers may have an impact on mortality in stable angina outside the context of acute MI. 10 Beta-blockers also affect mortality in the treatment of heart failure.11–15
Current literature contains few large long-term studies, but many small studies of short duration. Thus, a systematic review and meta-analysis may elucidate the impact of beta-blockers on prognosis as the individual small trials are underpowered to do so. The objective of this study was to assess the impact of beta-blocker administration upon the mortality rates of patients with stable angina by conducting a meta-analysis of all randomized controlled trials.
Methods
Eligibility criteria
Randomized controlled trials of at least three weeks duration involving either beta-blockers versus placebo or beta-blockers versus other antianginal drugs separately were included. Trials that only examined patients following MI and those that included patients with unstable angina were excluded. Paediatric patients and those with non-cardiac chest pain were also excluded.
Outcome measures
Cardiovascular mortality was selected as the primary outcome measure.
Search strategy
The published literature was searched from 1966 to 2009 in online databases, including MEDLINE, EMBASE and CINAHL; major cardiology journals were also hand searched for the relevant articles. The search was limited to English language trials because we needed to access the full text of the article to determine if there were any deaths in trials where the primary outcome measure was not cardiovascular mortality. Full articles were retrieved in all studies that: (1) examined patients with stable angina; (2) compared beta-blockers with placebo or other antianginal medication; and (3) used random allocation to comparison groups. We searched www.clinicaltrials.com in order to find unpublished clinical trials.
The following MEDLINE search strategy was used and adapted for the different databases, 16 and the search terms are given in Supplementary Table 1.
Statistical analysis
Peto's method17,18 was used for calculating combined relative risk using the fixed effects model to identify the pooled relative risk and 95% confidence intervals (CIs). Review Manager 19 was used to create forest plots and do statistical calculations. We separately considered and performed tests of heterogeneity (χ2-test) for trials included under both groups of trials (beta-blocker versus placebo, beta-blocker versus other) as well as within different cardio-specificities of beta-blockers included in the trials. We constructed a funnel plot to look for important publication bias.
Results
The literature search identified 2700 relevant publications. All full-text articles that fulfilled our inclusion criteria were reviewed. Of these, 29 trials of beta-blockers versus placebo and 60 trials of beta-blockers versus other antianginals were identified that met the criteria (see Methods section).
Beta-blockers versus all other (placebo and antianginals)
We pooled all 89 trials (n = 21,674 patients) that were identified, assessed beta-blockers against all other controls and recorded the primary outcome measure. There was no evidence of a difference in cardiovascular death (Peto odds ratio [OR], 0.97; 95% CI, 0.86–1.09) that the test for heterogeneity (χ2= 25.09, df = 23 [P = 0.35]; I2= 8%) suggested that any heterogeneity if present was small, meaning that the combination of trials does not introduce significant error. We found that the test for overall effect was non-significant: Z = 0.54 (P = 0.59). Overall, this combined analysis does not provide any evidence that beta-blockers have a significant impact on mortality in patients with stable angina (Figure 1).
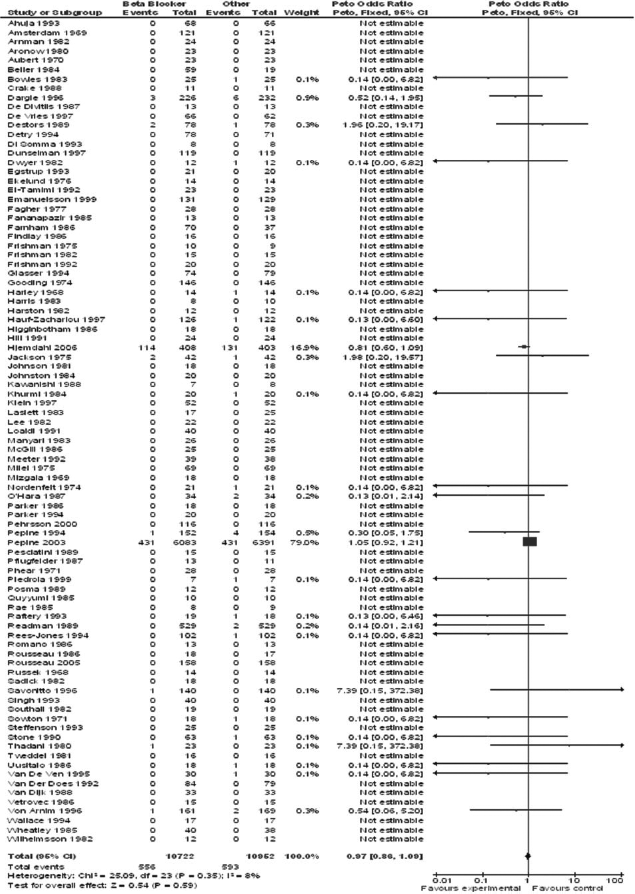
Forest plot of beta-blockers versus all controls. Point estimate is 0.97 (CI, 0.86–1.09), implying that there is unlikely to be an impact of beta-blockers when compared with all other controls and that the benefit is less than 14%, hazard less than 9%
The funnel plot (Figure 2) shows a distribution of trials on both sides of the midline, suggesting that there is no important publication bias.
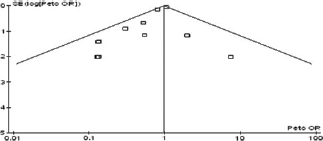
Funnel plot of beta-blocker versus all controls. The funnel plot used to detect publication bias has a scatter roughly around the midline
Beta-blockers versus placebo
We pooled the 29 trials of beta-blockers (n = 2315 patients) that assessed beta-blockers of varied cardioselectivity against placebo and recorded the primary outcome measure. The mean trial length was 13 weeks, median length was eight weeks. There were few very long-term studies and most were under six months in duration. We found a Peto OR of 0.42 (95% CI, 0.15–1.21) (Figure 3). The point estimate suggests that beta-blockers may have a positive impact on mortality; however, it does not prove such a relationship because the CIs overlap unity. We found that heterogeneity: χ2= 5.56, df = 7 (P = 0.59); I2= 0%. The I2 test suggests that heterogeneity if present is small, which means that the combination of trials does not introduce significant error. The test for overall effect was Z = 1.60 (P = 0.11).
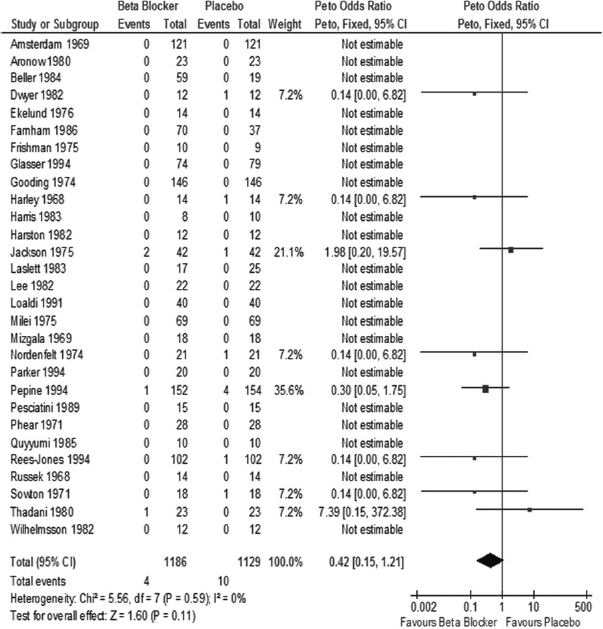
Forest plot of beta-blockers versus placebo. Point estimate is 0.42 (CI, 0.15–1.21), suggesting that there may be a benefit of beta-blockers compared with placebo as large as 85%, but the hazard may be as high as 21%
By design, cardioselective beta-blockers and non-cardioselective beta-blockers were considered separately.
For cardioselective beta-blockers the Peto OR was 0.24 (95% CI, 0.05–1.06), whereas for non-cardioselective beta-blockers the Peto OR was 0.75 (95% CI, 0.17–3.32), though both CIs overlap unity. However, because the point estimate for cardioselective beta-blockers is lower and the CIs only just overlap unity, there is a strong suggestion that cardioselective beta-blockers may have an impact on mortality. This remains unproven.
Furthermore, the test for overall effect is Z = 1.89 (P = 0.06), almost at the level of statistical significance (P < 0.05), compared with non-cardioselective beta-blockers where the overall effect is Z = 0.38 and the P value is much larger (P = 0.70). The test for subgroup differences (χ2 = 1.04, df = 1 [P = 0.31]; I2= 4.1%) suggested that there is no statistically significant difference between the subgroups.
There is little evidence of heterogeneity within trials for cardioselective beta-blockers (χ2= 0.23, df = 2 [P = 0.89]; I2= 0%), as well as trials for non-cardioselective beta-blockers (χ2= 4.20, df = 4 [P = 0.38]; I2= 5%). This again suggests that the combination of trials does not introduce significant error into the study.
The funnel plot (Figure 4) shows that there are trials on both sides of the midline, suggesting that significant publication bias is absent, although the relatively small number of trials in this component of the study and the relatively few events in most trials mean that the findings for this component are not conclusive.
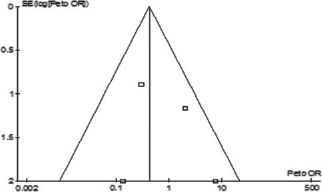
Funnel plot of beta-blockers versus placebo. The funnel plot used to detect publication bias has a scatter roughly around the midline
Beta-blockers versus other antianginals
We pooled the 60 trials of beta-blockers (n = 19,343) which assessed beta-blockers against other antianginal medications. A priori, we separately considered cardioselective and non-cardioselective beta-blockers versus other antianginals, and we performed a separate analysis within the antianginals (calcium channel antagonists versus the remainder of antianginals). The mean trial length was 19 weeks, while the median length of trial was eight weeks. We found a Peto OR of 0.98 (95% CI, 0.86–1.10; test for overall effect, Z = 0.38 [P = 0.70]). The OR was very close to unity, and the CIs overlapped unity, which suggests that beta-blockers have similar impact on mortality in patients with stable angina when compared with other antianginals. The test for overall effect also suggested that the difference in impact was not statistically significant (Figure 5).
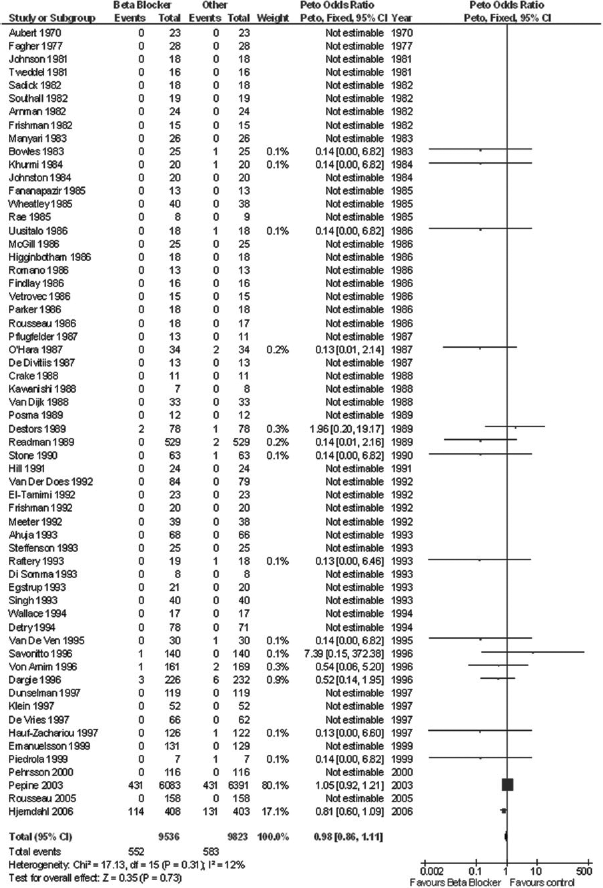
Forest plot of beta-blockers versus all other antianginals. Point estimate is 0.98 (CI, 0.86–1.11), implying that there is unlikely to be an impact of beta-blockers when compared with calcium channel blockers and that the benefit is less than 14%, hazard less than 9%
The test for heterogeneity (heterogeneity: χ2= 17.13, df = 15 [P = 0.31]; I2= 13%) showed that overall there was no significant heterogeneity as a source of error when we combined the trials.
When considering cardioselective beta-blockers, the Peto OR was 0.99 (95% CI, 0.87–1.21; test for overall effect, Z = 0.19, P = 0.85), whereas for non-cardioselective beta-blockers the Peto OR was 0.33 (95% CI, 0.09–1.21; test for overall effect, Z = 1.68 [P = 0.09]), but both CIs overlapped unity.
With trials for cardioselective beta-blockers (χ2= 10.81, df = 9 [P = 0.28]; I2= 18%) and trials for non-cardioselective beta-blockers (χ2= 3.58, df =5 [P = 0.61]; I2= 0%), the I2 value and χ2 suggested that the extent of heterogeneity was small, again suggesting that the combination of trials did not introduce significant error. The funnel plot (Figure 6) showed a roughly equal distribution of plots on both sides of the midline, which suggested that there is no important publication bias.
Funnel plot of beta-blockers versus all other medications. The funnel plot used to detect publication bias has a scatter roughly around the midline
Discussion
Our findings show that there is no evidence of a statistically significant effect of beta-blockers upon mortality in patients with stable angina. The analysis excluded studies in the context of acute MI. Overall, the point estimate for beta-blockers versus control is 0.97, and the CIs are narrow. These exclude a benefit of 15% or greater and hazard of 10% or greater. When considering beta-blockers versus other antianginals, the point estimate is closer to unity at 0.98, and the narrow CIs exclude a benefit of 14% or greater and hazard of 11% or greater.
Based on the trends and the point estimates, the findings raise the possibility that cardioselective beta-blockers may be superior to non-cardioselective beta-blockers when compared with placebo and that beta-blockers may be better than nitrates or other non-calcium channel antagonists. In contrast to the overall findings, the point estimate is 0.53, but the CIs are wide and they cross unity. Further study is needed to confirm or refute these possibilities, although it may be difficult to obtain funding support for a trial of sufficient size to compare beta-blockers with placebo. For the comparison of beta-blockers with other antianginals, one large trial (APSIS) dominated the findings. Larger-scale trials using non-cardioselective beta-blockers are needed to confirm this.
Since 1999, when the last meta-analysis 6 was performed, we have also found that even with the inclusion of more recent trials there is no significant impact on mortality in patients with stable angina when compared with calcium channel blockers.
The strength of our study is that it is up to date and comprehensive. No other meta-analysis has been performed on this topic within the last decade. Our study specifically excluded beta-blocker use in the context of acute MI because we wanted to identify the impact of beta-blocker use in chronic cardiovascular conditions such as stable angina. Furthermore, beta-blockers following MI are already known to be effective. We endeavoured to be as inclusive as possible. All trials included were randomized, although some did not elucidate the randomization process. We have excluded observational or nonrandomized studies as treatment effect cannot be reliably interpreted from such studies.
Small unpublished trials are possible sources of error as they were not included. However, they are unlikely to influence the overall result. Only full English language texts were used in our meta-analysis because we had to examine each study's secondary outcome measures as part of our selection process.
Beta-blockers act to improve mortality in heart failure by reducing the circulating levels of catecholamines and reducing activation of the renin-angiotensin system. Because of the observed impact of beta-blockers on mortality after MI, it is possible that the pathophysiology of heart failure and the conditions following MI share similar pathways. These raise the possibility of new treatment strategies for both.
Conclusion
We have found no evidence that beta-blockers have a statistically significant effect on mortality in patients with stable angina. The trials published to date cannot exclude the possibility that cardioselective beta-blockers differ from non-cardioselective beta-blockers when compared with placebo. Although further study is merited, this issue is unlikely to be resolved as randomized studies would need to be very large.
Supplementary material
The supplementary material accompanying this article can be found online at: http://smj.rsmjournals.com.
Footnotes
Acknowledgements
We would like to thank Dr Steff Lewis for her support with statistical analysis, and Sheila Fisken, the Medical Librarian.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.