
Abstract
The authors present a rare case of ventriculitis secondary to cerebro spinal fluid (CSF) colonization with Escherichia coli species in a 65-year-old woman. Passage of bacterial organisms from the lumen of the gastrointestinal tract to the bloodstream or lymphatic tissue is known as translocation. Once in the bloodstream, particular bacteria are able to cross the blood–brain barrier and migrate to CSF. Elective abdominal surgery, intestinal obstruction, colorectal cancer, ischaemic reperfusion injury and pancreatitis have all increased the risk of this phenomenon. This account highlights particular events in presentation and management of such a case, followed by a brief literature review.
Case presentation
A 65-year-old lady initially presented with urinary retention, hypotension and peripheral oedema. Her past medical history was significant for an anterior resection, hysterectomy and bilateral salpingo-oophorectomy 14 years previously for advanced recto-sigmoid carcinoma. The procedure was followed by adjuvant radiotherapy and reversal of her surgery two years later. She developed radiation-induced strictures with multiple adhesions (radiation enteritis), which resulted in hospitalization for small bowel obstruction on two separate occasions. These latter events settled with conservative measures. A rectal stricture was pending endoscopic dilation on an outpatient basis.
As the acute presenting condition resolved with antimicrobials and fluid resuscitation, there was progressive distension of the abdomen with accompanying low-volume loose stool. A plain radiograph showed distended small bowel loops (Figure 1) with a moderately distended large bowel. Computed tomography (CT) scanning of the abdomen confirmed the presence of closed-loop small bowel obstruction (Figure 2). Nasogastric drainage of stomach contents was instituted together with intravenous fluids and antimicrobial treatment. Investigations revealed markedly elevated inflammatory markers and blood cultures grew Escherichia coli organisms and coliforms.

Plain abdominal radiograph showing locally distended loops of small bowel present in the mid- and lower abdomen in keeping with underlying obstruction

Computed tomography scan of the abdomen showing marked gas and fluid distension of the mid and distal small bowel
The patient showed signs of improvement over 2–3 days and arrangements were in place for her endoscopic rectal dilation. Over a course of 24 hours, however, a gradual deterioration in Glasgow Coma Scale was noted and neurological examination revealed right-sided facial weakness. CT scanning of the brain showed gas and debris in the ventricles, with no lesions to suggest a possible cerebro-vascular accident (Figure 3). A diagnosis of ventriculitis secondary to translocation of enteric bacteria from a closed-loop small bowel obstruction was made. Intravenous piperacillin/tazobactam was promptly administered and the patient was transferred to neurosurgical care.
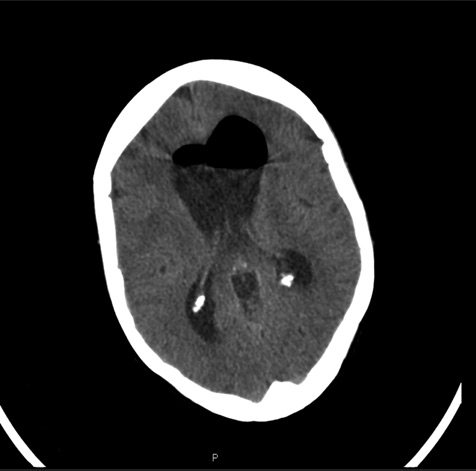
Computed tomography scan of the brain showing marked intraventricular gas in the lateral ventricles and associated ventricular dilation
An external ventricular drain was placed and samples of cerebro spinal fluid confirmed the presence of E. coli. She was started on appropriate antimicrobials with clinical improvement evident after 72 hours. A ventriculo-peritoneal shunt was subsequently inserted. Her convalescence was complicated by grand mal seizures, which are currently well controlled with appropriate anti-epileptics. A remarkable recovery is otherwise observed.
Discussion
A relatively rare case of bacterial translocation from the bowel to the cerebral ventricles is presented. The gut has complex metabolic and immunological roles beyond digestion. 1 Classically, it also functions as a barrier to prevent the spread of intraluminal bacteria and endotoxins systemically. 2
The number of bacteria present within the gut lumen is usually around 1012 per millilitre of faeces. 3 These organisms make-up most of the flora in the colon and 60% of the dry mass of faeces. The functions of intraluminal bacteria are multiple. However, when the gut lining is overwhelmed or impaired, bacterial translocation may ensue. 4 In relation to E. coli, bacterial counts within the blood of >10 3 CFU (colony-forming units)/mL were found to result in significantly more meningitis cases than those with bacterial counts of <10 3 CFU/mL. 5
The degree of bacteraemia alone is not sufficient for the development of meningitis. Recent studies with E. coli have shown that several structures are necessary for crossing the blood–brain barrier, 6 such as specific membrane proteins and glycoproteins (specifically the K1 E. coli structure, outer membrane protein A7,8 and invasion of brain endothelial cell proteins A, B and C 3 ).
Ventriculitis is the inflammation of the ventricles within the brain and has been shown to occur through the involvement of the ependymal lining following meningeal inflammation in around 30% of patients, 9 most commonly affecting infants.
Underlying mechanisms of how and under what circumstances bacteria contained within the gut translocate across the mucosal barrier have been studied extensively by Deitch and Berg. 5 They suggest that translocation is prevented by firstly, the presence of indigenous microflora controlling bacterial overgrowth, secondly, an intact intestinal epithelial barrier and thirdly, normal host immune defences. Therefore, failure or disruption of these protective mechanisms can potentially lead to systemic infection. Around 15% of elective surgical patients experience bacterial translocation, occurring most frequently in those with intestinal obstruction and those who are immunocompromised. 3 Colorectal cancer, ischaemic reperfusion injury and pancreatitis 4 can also be predisposing factors.
Our patient had a previous anterior resection followed by radiotherapy for carcinoma of the recto-sigmoid junction. A postoperative rectal stricture is postulated to have enhanced the degree of translocation, due primarily to subacute large bowel obstruction and pathological bacterial overgrowth. When superimposed by a closed-loop small bowel obstruction, significant translocation appears to have occurred. Bowel ischaemia or recurrent cancer as a source of translocation had been excluded in this lady, with the aid of CT. It is reasonable to assume that portal vein seeding to the liver would usually precede cerebral colonization in such a case, explained by the anatomy of the portal venous system.
In conclusion, patients with obstructive bowel symptoms and unexplained neurological deterioration may have cerebral sepsis. We present an unusual course of sepsis that deviates from the natural progression of portal pyaemia in patients with marked bacterial translocation from the gut.