
Abstract
Policy-makers consider telehealth to be a potential solution to delivery of care in rural Scotland. Telehealth can support patients in the community and may reduce emergency admissions to hospital. The Argyll & Bute telehealth initiative, which commenced in 2007, trialled home telehealth monitoring of patients with chronic obstructive pulmonary disease (COPD), and community- and surgery-based monitoring of general wellbeing and hypertension. An evaluation in 2010 assessed staff and patient satisfaction by questionnaire, impact on hospital and general practice attendance by case record review and detailed opinions on the programme by qualitative interviews with key staff. Home monitoring for COPD was associated with high levels of patient satisfaction and a reduction in hospital admissions and other health service contacts. Delays in implementation and some technical challenges compromised evaluation of the surgery and community initiatives. Patients and staff were generally enthusiastic but also identified potential barriers to development. This paper describes the implementation and outcomes of the initiative and identifies issues that clinicians embarking on telehealth programmes must consider: technical factors; governance and security; staff profiling and training; clinical outcomes; and scalability.
Introduction
Policy-makers regard telehealth as an essential component of future delivery of care in rural Scotland. 1 It has potential to improve patient outcomes in a range of different contexts.2–7 However, clinicians embarking on telehealth have to consider technical, organizational and clinical factors and recognize that successful implementation will involve changing conventional practice.
This paper focuses on a programme instituted in Argyll & Bute, which extends almost 100 miles north to south with 25 inhabited islands. Systems were introduced to allow home monitoring of chronic obstructive pulmonary disease (COPD) and community-based monitoring of hypertension and general wellbeing.
Morbidity and mortality from COPD in Scotland is high, 8 with over 200,000 patient consultations between 2007 and 2008. 9 Routine monitoring has shifted from general practitioners (GPs), with a marked increase in practice nurse (PN) contacts from 38,425 in 2003/2004 to 101,646 in 2007/2008. 9 Telehealth can support COPD patients at home 10 and can reduce hospital admissions,4,6,7,11–13 with patients tending to comply with monitoring. 14 There is also evidence that telehealth monitoring is beneficial in patients with hypertension 15 and in promoting general wellbeing. 16
This paper describes an evaluation performed in 2010, three years after the inception of the Argyll & Bute programme. It illustrates practical challenges and benefits and provides recommendations for clinicians engaged in future programmes.
Methods
The Argyll & Bute Telehealth Project evolved from an existing telecare service supported by the Scottish Government Joint Improvement Team. In May 2007, several telehealth companies were invited to present to a project steering group.
The project aims were to expand the use of technology to support long-term conditions; to develop local staff expertize use in the use of remote monitoring in patient care; to expand the specialist knowledge available by developing practitioners with a special interest in the project areas; to assist patients to manage their long-term conditions; and to a link this work to a reduction in crisis admissions to hospital.
The steering group wished to pilot home monitors for COPD and surgery and community telehealth monitors in accessible locations. A delay in implementation ensued as the commercial supplier initially chosen was subsequently de-selected due to concerns regarding procurement. A new supplier (Telehealth Solutions Ltd., Watford, UK) was engaged to provide equipment and logistical support for the initiative. Time lost in negotiations with the original supplier was significant, as discussed later.
Three types of systems or ‘Pods’ were installed: home monitoring, surgery monitoring and community monitoring. Home Pods were installed for 17 COPD patients in March 2009 with touch-screen facilities to enable daily clinical monitoring. Symptom reports and measures such as oxygen saturation were sent by wireless or broadband to the Telehealth Solutions secure server maintained behind the NHS firewall. Nominated community nursing teams checked a website daily and were alerted to changes in the patient's condition.
Touch-screen surgery Pods for general health monitoring were installed in general practices in Oban and on Bute, configured to transfer patient data instantaneously into the surgery's electronic patient record (EPR). Community Pods were installed in sheltered housing in Oban and in a community hall on the Isle of Luing. The Pods enabled patients to record their own physiological measurements including weight, body mass index, oxygen saturation, pulse and blood pressure. Each patient had swipe-card access to their own protocol. In the sheltered housing complex, the protocol gathered responses about general health as well as hypertension. Data were transferred onto a secure, NHS firewalled website for health professionals (primarily community nurses) to review. Results outside of the set parameters alerted community nursing teams. Community and surgery Pods became operational in October 2009, but full connection to the EPR had not occurred at evaluation.
Evaluation took place in early 2010. Questionnaires (one per subject, no reminders) were distributed to patients, staff and carers, asking project-specific questions together with an adapted version of the Client Satisfaction Questionnaire (CSQ-8) 17 and a free text response. For COPD patients, hospital admissions, general practice and emergency attendances were recorded for comparable nine month periods before and after installation of the Pods. Due to the numbers involved, formal statistical testing was not appropriate.
Ten qualitative interviews were conducted with healthcare professionals involved in the programme, including a general practitioner, three community nurses, a specialist practice nurse, two general practice managers, a respiratory nurse specialist, telehealth project manager and a sheltered housing warden.
A semi-structured qualitative interview guide was developed, informed by an eHealth Implementation Toolkit 18 designed to identify potential barriers and facilitators to embedding eHealth innovations. Key themes include ‘The Intervention’ (impact on clinical practice/ease of use of the system), ‘The Culture’ and ‘Context’ within which it is being implemented and ‘The Workforce’ (impact on workflow/work pattern and relationship between different staff groups).
Qualitative interviews lasted approximately 40 minutes and were digitally recorded with participant consent, transcribed verbatim, and analyzed descriptively using a framework approach.
19
The principles of the Normalization Process Model were applied during analysis.
20
This model helps to describe why some eHealth technologies become part of routine practice, while others do not.
21
It is defined by four constructs:
Interactional workability or ‘how is the work done?’ Relational integration or ‘how well does the system fit the work?’ Skill-set workability or ‘who does what and can they?’ Contextual integration or ‘how the organization helps or hinders’.
Results
There were considerable delays from inception of the project (2007) until the Pods were installed: March 2009 for COPD and October 2009 for community and surgery Pods. This was partly due to the enforced change in equipment supplier.
Quantitative results
Usage
Frequency of logging home telehealth recordings versus target was almost 100% for COPD patients, while the community systems, which had only been established for a short period, were less well used compared with target: 38% on Luing and 51% in the sheltered housing complex.
Satisfaction
Users of the Pods were generally older people (range, 61–102 years). Response rates for satisfaction questionnaires were: COPD patients, 77%; hypertension, 50%; wellbeing, 71%; staff, 86%; and carers, 50%. General satisfaction was high for all groups, particularly patients with COPD. Mean (standard deviation) CSQ-8 scores were 29 (3) for COPD patients, 23 (2) hypertension patients and 25 (3) for wellbeing; the maximum possible score is 32. Patients felt comfortable and safe (Figure 1) using the technology, found it easy (Figure 2) and felt it improved self-awareness and was appropriate for use in a remote and rural setting (Figure 3).

Patient perceptions on ease of use of telemonitoring

Patient perceptions of safety of telemonitoring
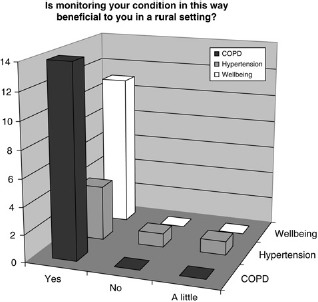
Patient perceptions of value of telemonitoring
Clinical impact
For COPD patients, comparing time periods March–November in 2008 and 2009 (i.e. pre/post installation), there was a reduction in GP visits, accident and emergency attendances and hospital admissions (numbers and bed occupancy) related to COPD (Table 1). Clinical impact of community and surgery Pods was not measured due to the short period of implementation.
All contacts, GP or district nurse/PN visits and hospital admissions data (numbers and bed days)

Qualitative results
COPD monitoring
Qualitative feedback was generally positive, although a number of ‘normalization’ issues concerning training, communication and integration with existing professional work patterns were identified.
Most interviewees felt home telehealth monitoring for COPD was appropriate for community nurses to manage and could be integrated into established working patterns, demonstrating a high level of ‘relational integration’. The ‘skill set workability’ was appropriate for community nursing teams, providing an opportunity to increase their knowledge of COPD. Most felt it was appropriate for rural patients to be monitored at home and that telemonitoring promoted self-management:
I think they are more aware of their health…they are thinking about ‘how do I feel today?’ They're more aware of their illness and what to do and what not to do as the symptoms arise.
Despite initial concerns from some staff, home monitoring had good ‘interactional workability’, and the technology was described as ‘straightforward’ and easy to use. Regular interaction between nurses and patients took place:
Patients get much more appropriate and timely management of their condition doing telehealth because they're not so invisible’.
A number of technical implementation challenges were identified. Aside from the difficulties with the first supplier, time to install equipment and home broadband connections was underestimated, utilizing more staff resources and resulting in project delays.
Most respondents had concerns about impact on their current and future workload. The current workload was described as manageable; however, there were concerns expressed if the number of COPD patients using telehealth was to increase. The home COPD Pods affected community and district nursing workload in particular. This may impact upon future ‘skillset workability’.
It has certainly increased the pressure of the job because you are very much aware, with the alerts coming through daily. For example I didn't get to check my email until the afternoon, so if there is an alert coming in the morning and you haven't seen that until the afternoon …there is a little bit of pressure there thinking, you need to check them in the morning. It's not always feasible to do that.
Home monitoring of patients also disrupted some internal relationships between nursing staff. Some did not want to take on the extra responsibility of checking patient readings. Staff reported that training could be improved to enhance confidence.
Surgery monitoring
The potential of surgery telehealth monitoring had not been achieved, mainly due to the delay in establishing an EPR link. At the time of evaluation, surgery telehealth monitors were functioning without the electronic link to the EPR, impacting on the use of surgery Pods and on professionals’ enthusiasm for the technology in its current form, although potential future advantages were recognized:
Take our hypertensive patients; once a year we definitely need to see them because we need to assess their compliance with their medication, to check their bloods, we need to check their weight and do all their lifestyle details etc. But the in-between check when they are needing their blood pressure done could be done easily by the Pod… we have eleven hundred people with hypertension, so we could be reducing our unnecessary consultation rate considerably.
Community monitoring
There were a number of challenges associated with community telehealth monitoring. On Luing, there were broadband difficulties and installation delays. In Oban, the sheltered housing was located close to the GP surgery, the ease of access to which reduced the incentive to use telehealth. However, the system may be appropriate in similar settings farther from a GP surgery. At the time of evaluation, it was too early to assess any potential clinical benefit.
Discussion
The operation of the telehealth initiative in Argyll & Bute has been generally welcomed, with early indications that clinical benefits may be gained from home monitoring of COPD. From a wider perspective, this evaluation highlights a range of considerations for clinicians adopting telehealth approaches to delivery of care. These are discussed in turn.
Technical issues
Shared understanding and close collaboration with the equipment provider is essential. In this project, a change of supplier was required, resulting in a significant delay in implementation. Connectivity is important, both for internal and external links. In this project, delays in linking the surgery Pods to the EPR systems (internal connectivity) meant that data had to be transferred manually between systems, leading to underuse in the first instance, although connectivity was later established. In relation to external connectivity, broadband provision in Scotland's rural areas remains poor, 22 hampering systems that require reliable bandwidth provision. In this project, broadband linkage to Luing was initially unreliable, a major potential disincentive to new users of the system. Recently announced initiatives to enhance rural broadband provision may overcome these problems but will require close cooperation between healthcare providers, government, commercial and enterprise agencies.
Costs
Due to the small numbers involved, a formal cost-benefit analysis was not carried out. However, indicative costs for the delivery of telehealth were as follows. The home Pods capital costs were £1100 per unit, including peripherals (e.g. for measurement of oxygen saturation), training and installation. Operating costs were £500 per annum per unit. For the surgery and community Pods, capital costs were £7130 per unit, including peripherals and a standalone blood pressure cuff, plus installation and training and swipe cards for access to the community pods. The operating costs for these pods were £1500 per Pod annum, including updates and use of the website for monitoring and security.
Governance and security
This is a particular concern for telehealth terminals located in community settings such as village halls and housing complexes. Some implementation delays in this project related to guaranteeing physical security of the equipment (e.g. placing the terminal in a locked cabinet) while ensuring appropriate access, and to compliance with NHS governance for data security. The latter added about five months to the implementation time in this project.
Staff profiling and training issues
Managing chronic disease while incorporating telehealth alters the interaction between patients and health care workers and changes responsibilities for staff. In this project, staff reported concerns that telemonitoring could impact on their conventional workload, since patients were empowered to make more frequent contacts with their healthcare providers. This effect will in part relate to the scale of any telehealth initiative. Training in the use of technology and in the revised mode of interaction with patients is essential, especially for those staff more peripherally involved with telehealth. Finally, changes in relationships between members of the healthcare team may occur and this needs to be explicitly considered in planning.
Clinical outcomes
Careful consideration must be given to anticipated clinical outcomes. In this project, the targets for the COPD patients included a general improvement in quality of care and a reduction in hospital admissions. Feasibility and operability of home monitoring in this setting was studied but it was not powered to test whether the observed reduction in hospital contacts is statistically significant, although it was consistent with findings of other published studies.4,6,7,11–13
Scalability
A major challenge for healthcare providers worldwide is to scale up from local projects to regional or national provision. In the UK, a number of recent initiatives address implementation of telehealth at scale, including the Whole System Demonstrator initiative in England,23,24 the Scottish Telehealthcare Action Plan, 25 and the Scottish Centre for Telehealth strategic framework. 26 Large-scale implementation may realize benefits in standardization of practice and economies of scale, but may result in a loss of autonomy and control among local practitioners, which may be a cause for concern in isolated rural communities.