
Abstract
Patients with physical problems related to the use of alcohol or drugs often present to general hospitals in an unplanned, emergency fashion. In 2005, the Kerr report concluded that fundamental changes were needed in our approach, shifting the emphasis from a reactive to a more proactive, prevention-based model in the treatment of acute medical conditions. We studied patients who had at least one alcoholor drug-related emergency admission, whose most recent admission was to Aberdeen Royal Infirmary and who, using the Scottish Patients at Risk of Re-admission and Admission (SPARRA) All Ages Tool, were thought to be at high risk of further emergency admission. We examined data sets derived from the National Health Service National Services Scotland Information Services Division, a Liaison Psychiatry database, data from the local psychiatric Patient Information Management System and data collected by the hospital alcohol liaison nurse to examine this group of patients further and consider the scope for any future intervention. Patients who have an alcoholor drug-related emergency admission to the general hospital are at increased risk of re-admission. A substantial proportion of these patients has come into contact with the psychiatric services, often attracting a substance misuse and/or personality disorder diagnosis. A significant proportion also presents in the context of self-harm. In conclusion, this group of frequent hospital attenders may be difficult to engage but may benefit from more proactive intervention, a more joined-up management approach and the development of an enhanced general hospital alcohol liaison service.
Background
In 2005, the National Framework for Service Change in Scotland and the ministerial response (Delivering for Health) called for a fundamental re-orientation in the way health care is delivered in Scotland.1,2 In summary, there was a desire to shift from a system geared towards reactive hospital-based treatments of acute conditions to a system founded on a preventive, anticipatory approach and the management of long-term conditions on a whole person rather than disease basis.
In order to further these aims, Information Services Division (ISD) developed Scottish Patients at Risk of Re-admission and Admission (SPARRA), a tool to allow prediction of an individual's risk of being admitted to a general hospital as an emergency within a given one-year period. 3 Risk prediction is undertaken for those patients who have at least one emergency admission over a three-year risk-calculation period. Based on this information, patients are divided into those at high risk (SPARRA score of ≥50) and those at low risk (SPARRA score of <50) of re-admission. Such risk prediction was initially only applied to patients aged 65 and over, but more recently the tool has been developed to apply to patients of all ages (SPARRA All Ages). 4 By identifying patients at high risk of re-admission, it is hoped that more proactive interventions can be developed in order to reduce the risk of re-admission and facilitate more appropriate long-term management.
Alcohol misuse has profound cost implications for both the National Health Service (NHS) in Scotland and wider Scottish society. The cost imposed upon the NHS in Scotland and Scottish society as a whole was estimated to be £95.6 million and £1.1 billion, respectively, at 2001/2002 prices. 5 Heavy drinkers have been identified as disproportionate users of acute hospital services (e.g. accident and emergency departments) and relative under-users of community services (general practioners [GPs], dentists and opticians). 6 Alcohol consumption contributes to hospitalization as a result of accidents, domestic and criminal violence, self-harm and the medical complications of longer-term organ damage induced by heavy drinking. 7
Aims of this pilot study
Following release of SPARRA All Ages in January 2009, it became apparent that patients with alcoholor drug-related general hospital emergency admissions feature highly in the group of patients at risk of re-admission. This association prompted an interest in exploring this relationship and the scope for further possible interventions in this particular patient group. In order to achieve this, a pilot study was set up between ISD and the Department of Psychological Medicine (Liaison Psychiatry) in Aberdeen to try to answer a number of questions:
Of those patients with at least one alcoholor drug-related emergency over a three-year period and whose most recent admission was to Aberdeen Royal Infirmary (ARI), how many are considered to be at high risk of re-admission over a subsequent one-year period? Of those patients, how many were referred during the three-year risk assessment period to liaison psychiatry and how many were referred to the alcohol liaison nurse (ALN)? How many patients were, during the three-year risk assessment period, admitted to a psychiatric hospital and what was the discharge diagnosis? How many patients had previous contact with the mental health services in Grampian and what was the nature of this contact? Is there scope for any future intervention that would enhance patient care and reduce the risk of re-admission to the general hospital? Would provision of routine SPARRA information relating to patients with alcohol or drug-related emergency admissions be of operational value to mental health services?
Method
Based on a three-year risk-calculation period (1 July 2006–30 June 2009), the SPARRA All Ages tool was used to predict which patients with at least one emergency admission and their most recent admission to ARI were at high risk of a further emergency admission over the ensuing one-year period (1 July 2009–30 June 2010). High risk was defined as a 50% or higher chance of being re-admitted. This was compared with the re-admission risk of patients who had at least one alcoholor drug-related emergency admission. All patients in the latter group were matched against data obtained from the Liaison Psychiatry departmental database to determine which proportion of patients, during the risk calculation period, had been referred to liaison psychiatry. The departmental liaison database provides information about referral source, reasons for referral, diagnosis as well as disposal. Referrals to general adult liaison psychiatry include patients who present following an episode of self-harm (age 14 and up), ward referrals (age 18–65) as well as outpatient referrals from general hospital practitioners (age 18–65). Furthermore, we identified which proportion of patients had been referred to the ALN at ARI. We also obtained SMR04 data from ISD to establish which proportion of patients had been admitted to a psychiatric hospital during the risk calculation period and what the discharge diagnosis was. We finally examined, based on data obtained from the psychiatric Patient Information Management System (PIMS) in Aberdeen, which high-risk SPARRA patients had any previous or ongoing contact with the psychiatric services in Grampian. We used SPSS version 15.0 for Windows (SPSS Inc., Chicago, IL, USA) in order to analyse the data.
Results
During the three-year risk-calculation period, a total of 44,576 patients (whose most recent admission was to ARI) had at least one emergency admission. Of those, 2265 patients (5.1%) were considered to be at high risk of re-admission, 5015 patients (11.2%) had at least one alcoholor drug-related emergency admission and of those, 426 patients (8.5%) were considered to be at high risk of a further emergency re-admission. Table 1 shows a comparison of these four groups of patients in terms of total number of emergency admissions as well as mean number of emergency admissions.
Total and mean number of emergency admissions in four different patient groups
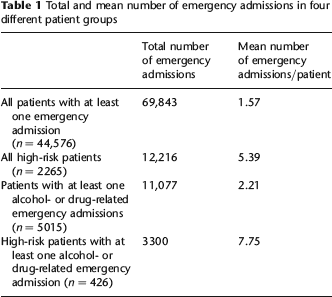
The mean SPARRA risk score in the high-risk group of patients who had at least one alcoholor drug-related emergency admission (N = 426) was 64.5 (range, 50–93; standard deviation [SD], 10.5). They had a mean number of 4.5 (range, 0–35; SD, 4.5) alcohol-related admissions and a mean number of 0.5 (range, 0.10; SD, 1.6) drug-related admissions. Two hundred and ninety-two patients (68.5%) were men and age ranged from 20 to 91 years (mean, 55 years; SD, 15.8). One hundred and thirty-one patients (30.8%) were over the age of 65. The mean age was higher in men (56.2 years) than women (52.1 years), but this did not reach statistical significance.
Referral to liaison psychiatry
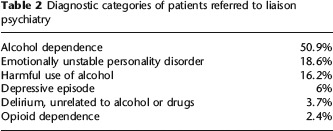
Of all 426 identified high-risk SPARRA patients, 117 (27.4%) had been referred to liaison psychiatry during the risk-calculation period, some patients on several occasions. These 117 patients generated a total of 381 referral episodes. Eighty-five patients were referred following an episode of self-harm (289 referral episodes, mean 3.4 episodes), 58 were referred as a ward referral (91 referral episodes, mean 1.6) and one patient was referred as an outpatient. These figures do not add up to 117 as some patients were referred both following an episode of self-harm and as a ward referral. Only nine patients over the age of 65 were referred as elderly patients are normally passed on to old age psychiatry unless self-harm is the main reason for referral. Eight out of those nine patients were indeed referred following an episode of self-harm. When the original sample of 426 patients was restricted to those under the age of 65 (n = 295), the proportion referred to liaison psychiatry increased to 36.6%.
Table 2 shows the most common psychiatric diagnoses, expressed as percentages of all liaison psychiatry referral episodes (n = 381).
Diagnostic categories of patients referred to liaison psychiatry
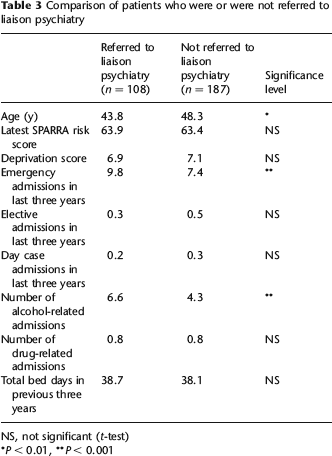
A comparison of patients who were and were not referred to liaison psychiatry is summarized in Table 3.
Comparison of patients who were or were not referred to liaison psychiatry
NS, not significant (t-test)
P < 0.01,
P < 0.001
Patients who were deemed to be at high risk of re-admission and who had also been referred to liaison psychiatry were younger, had more alcohol-related admissions and more emergency admissions. The two groups did not differ significantly in terms of SPARRA risk score, deprivation score, number of drug-related admissions, elective or day case admissions or total number of hospital bed days.
Inpatient psychiatric admissions
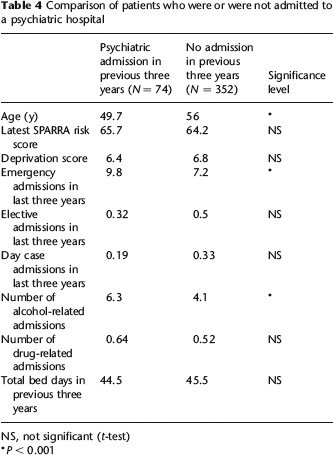
Seventy-four of all 426 patients (17.8%) had been admitted to a psychiatric hospital during the three-year risk assessment period at least once. The number of psychiatric admissions ranged from 1 to 14 (mean, 2.1; SD, 2.0). There was a total of 155 psychiatric admissions altogether. Patients who were admitted were more likely to have been referred to liaison psychiatry during the three-year period (P < 0.001, chi-square).
A comparison of those patients who were admitted with those who were not is summarized in Table 4.
Comparison of patients who were or were not admitted to a psychiatric hospital
NS, not significant (t-test)
P < 0.001
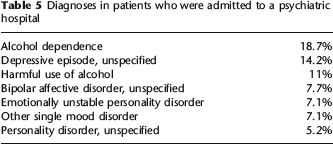
The most frequent psychiatric discharge diagnoses are summarized in Table 5.
Diagnoses in patients who were admitted to a psychiatric hospital
Contact with local psychiatric services
By obtaining relevant data from the PIMS at Royal Cornhill Hospital, we were able to establish that of all 426 identified patients, 324 (76%) had been referred to the local mental health services before (from 1995 onwards). The number of referrals ranged from one to 66 (mean, 6.7; SD, 9.3). Two hundred and sixty-six patients (62.4%) had been referred prior to the risk calculation period and 267 (62.7%) had a referral falling within the risk calculation period. Looking at the five most recent referrals revealed that such referrals were most commonly made by patients’ GPs (51.7%) followed by general hospital referrals (34.0%). Patients were most commonly referred to the Substance Misuse Service (29.7%), followed by Liaison Psychiatry (27.2%) and Community Mental Health Teams (21.8%).
Contact with ALN
Seventy patients (17.4%) were referred during the risk assessment period (1 July 2006–30 June 2009) to the ALN. Another 45 patients were referred to the ALN outside this time window, bringing the total number of referrals to 115 (27%). The ALN had a prolonged period of sick leave during the risk-calculation period leading to the suspension of this service. It is therefore likely that referral numbers would have been significantly higher.
Discussion
In the following discussion, we will address each of our original research questions in turn:
Question 1
Five thousand and fifteen patients had at least one alcoholor drug-related emergency admission to ARI during the risk-calculation period. Of those, 426 patients (8.5%) were considered to be at high risk of a further emergency re-admission. A sizeable number of patients with alcoholor drug-related emergency admissions were thus considered to be at increased risk of re-admission.
Question 2
Of these 426 patients, 117 (27.4%) had been referred to liaison psychiatry during the risk-calculation period, with alcohol dependence and personality disorder being the most frequent diagnoses. A similar proportion (27%) had previously been referred to the ALN. An alcohol problem had therefore been recognized in a considerable number of patients and had prompted a referral.
Question 3
Seventy-four (17.8%) patients were admitted to a psychiatric hospital during the three-year risk-assessment period at least once, with the most common discharge diagnosis being alcohol dependence. Three hundred and twenty-four (76%) patients had previously been referred to the local mental health services (1995 onwards). The most common type of referral was from the GP to the Substance Misuse Service. In other words, many people in the identified high-risk group were known to the mental health service, most commonly in the context of their substance misuse problem.
Patients with substance misuse disorders are at risk of developing physical complications which will require admission to a general hospital bed. They are also more likely to engage in self-harming behaviour, behaviour which can be compounded by the presence of personality difficulties. In our group of patients, previous psychiatric contact was associated with a higher number of emergency admissions, but the available data did not allow us to determine any direction of causality. It is likely that both contact with the psychiatric services and emergency admissions to a general hospital are associated with the severity of a patient's substance misuse disorder and the extent of any resulting social disruption and decline.
Question 4
What steps can be taken to decrease the risk of patients being re-admitted to the general hospital and to develop a more proactive approach to their care? Our data did not allow us to determine how well patients engaged with any psychiatric contact when this was offered and whether this was associated with the risk of general hospital re-admission. A proportion of patients were seen by the ALN during their stay in the general hospital, and strengthening of this service should lead to an improved outcome for some patients.
Question 5
Flagging frequently admitted patients to the alcohol liaison service by making SPARRA data available could help to promote a more proactive approach with interventions aimed at reducing the risk of further re-admissions, such as relapse prevention work and active encouragement to keep outpatient appointments. Admission to the general hospital constitutes, at least for some patients with substance misuse disorders, a point of considerable crisis and can offer a fertile opportunity for behaviour change. Active and early intervention and follow-up coordinated by the local alcohol services should therefore be of benefit. For those patients who have advanced and often multiple organ damage and who are frequently admitted to the general hospital, abstinence is likely to be the only realistic goal. This goal should be reinforced by explanation of the disease progress, the results of tests and an appraisal of the likely prognosis.
Given the scale of the problem, however, it is unlikely that an alcohol or psychiatric liaison service alone can have a decisive impact. Further training of general hospital staff in substance misuse related issues is clearly important. The Scottish Government has set a HEAT target for the delivery of brief alcohol interventions with targeted areas such as accident and emergency departments as well as antenatal care. 8 Crawford et al. 9 demonstrated that patients who attended the accident and emergency department at St Mary's Hospital in London and who were subsequently referred to an alcohol health worker reduced their alcohol consumption; their visits to the accident and emergency department were also reduced over a one-year follow-up period.
In Grampian (as is the case in other regions in Scotland) psychiatric and medical case-notes are held separately and, as a consequence, mental health staff have limited and in some cases no awareness of patients’ presentations to the general hospital. Likewise, general hospital staff may know little about any concurrent mental health treatment or previous efforts to engage a patient in such treatment. We would suggest that ready, ideally electronic, access to concurrent psychiatric or medical information is important and that this can foster a more joined-up approach to the management of patients with substance misuse problems and enhance communication between services.
Finally, we would like to stress the importance of global measures to influence the availability and consumption of alcohol within the Scottish population (e.g. introduction of a basic unit of alcohol price). It is likely that this will have a significant impact on the prevalence of alcohol-related harm and use of general hospital resources. We feel that it is important that the discussion and implementation of such measures remain high on the political agenda and are actively pursued.
The authors are planning to analyse re-admission data for the period (1 July 2009–30 June 2010) once available. This will help to assess the validity of the risk prediction tool and may provide further insight into what if any intervention might prove helpful for this patient group.