
Abstract
Infiltrating syringomatous breast adenoma is an uncommon mammary neoplasm composed of angulated glandular structures with a variable amount of epidermoid differentiation which proliferate in a background of dense collagenous stroma. The patient presented with bilateral hardness and oedema of the nipples. Ultrasound and mammography revealed microcalcifications in retromammilary regions of both nipples. Histological examination of the resected specimens showed angulated glands and solid cords, lined by an inner layer of epithelial cells and an outer layer of myoepithelial cells, immersed in desmoplastic stroma. Within the solid cords reminiscent of squamous cells, occasionally aggregated in keratinizing cysts were found. To the best of our knowledge this is the first described case of bilateral infiltrating syringomatous breast adenoma with synchronous presentation. Infiltrating syringomatous adenoma is a rare lesion. A finding of infiltrating syringomatous adenoma in one breast should prompt careful examination of the opposite breast with adequate follow-up.
Keywords
Introduction
Infiltrating syringomatous breast adenoma is a rare, benign, infiltrating neoplasm of eccrine origin located in the dermis of the areola and nipple. 1 It is composed of angulated glandular structures with variable amounts of epidermoid differentiation, which proliferate in a background of dense collagenous stroma. After initial description, more than 30 cases of syringomatous breast adenoma have been reported in the literature. 2 In the literature, only one case of bilateral infiltrating syringomatous breast adenoma with asynchronous clinical presentation was described. 3 This is the first case report to describe bilateral, synchronous presentation of this rare breast adenomatous lesion which may mimic carcinoma clinically and radiographically.
Case presentation
Medical history
A 58-year-old woman presented with hardness and oedema of both nipples. Physical examination showed bilateral mastopathy of mild degree.
Clinical features
Mammographic examination showed microcalcifications in both nipples and retromammilary regions (Figures 1a–b). Ultrasound revealed microcalcifications in both nipples and retromammilary regions, and bilateral heterogeneous zones with dorsal attenuation in retromammilary area (Figures 1c–d). Axillary ultrasound showed no abnormalities. Ultrasound-guided fine-needle aspiration of both lesions was performed. Cytological analysis showed aggregates of atypical epithelial cells and microcalcificates which were consistent with carcinoma.
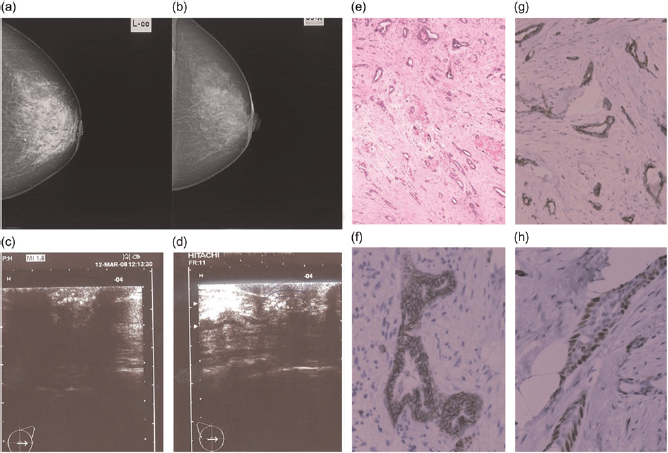
(a–b) Mammographic examination showed microcalcifications in both nipples and retromammilary regions. (c–d) Ultrasound revealed microcalcifications in both nipples and retromammilary regions and bilateral heterogeneous zones with dorsal attenuation in retromammilary area. (e–h) Histological examination showed angulated glands and solid cords, lined by an inner layer of epithelial cells and by an outer layer of myoepithelial cells, immersed in desmoplastic stroma. (e) Haematoxylin/eosin ×40, (f) E-cadherin (×200), (g) p63 (×200) and (h) CK5/6 (×200)
Differential diagnosis
The differential diagnosis includes tubular carcinoma, nipple adenoma and low-grade adenosquamous carcinoma.
Operative findings
Surgical intraoperative biopsy of both retromammilary regions was performed. Intraoperative histological analysis led to differential diagnosis of low-grade adenosquamous carcinoma or infiltrating syringomatous adenoma.
Pathological examination
Tumour was found on the resected edge of both specimens, and wider excision was performed. Histological examination of the intraoperatively received specimen showed angulated glands and solid cords, lined by an inner layer of epithelial cells and by an outer layer of myoepithelial cells, immersed in desmoplastic stroma (Figure 1e). Within the solid cords, reminiscent of squamous cells, occasionally aggregated in keratinous cysts, were present. In the subsequently received breast tissue there was residual tumour tissue in both received specimens 1 cm from the resected edge. The overlying skin and both nipples were without abnormalities. Immunohistochemically both tumours were ER, PgR, HER-2/neu, CK20, CD117, S-100 and p53 negative, and CK 5/6, CK7, actin, p63 and E-cadherin positive (Figures 1f–h).
Outcome, prognosis and follow-up
The patient made rapid recovery and was discharged on the eighth postoperative day. The patient was followed up at week 1 and months 1, 3 and 12. After that she was followed up every six months for two years, and then once a year. There were no complications and disease relapse.
Discussion
Infiltrating syringomatous adenoma is defined as locally recurrent and locally invasive tumour of the nipple/areolar region of the breast showing sweat duct differentiation. It is composed of infiltrating glandular structures and solid cords of cells with overt squamous differentiation.1–3 To the best of our knowledge the presented case is the second reported case of bilateral occurrence of this adenomatous lesion, but the first report of synchronous bilateral presentation and patohistological confirmation. In the case reported by Coulthard et al. 3 syringomatous adenoma of the left breast was found six months after excision of the same type of lesion in the right breast. Both lesions were initially reported as tubular carcinomas with foci of squamous differentiation. Interestingly, 20 months after the left breast surgery, a third lesion adherent to the overlying skin was noted in the region of the left axilla. Histological analysis of this lesion showed characteristics typical for benign syringoma, and histological sections of previously excised breast lesions were reviewed with subsequent revisions of initial patohistological diagnoses. 3 Infiltrating syringomatous adenoma of the nipple is often misdiagnosed because clinical presentation, mammographic and ultrasound findings may mimic carcinoma. 3 Some patients had undergone mastectomy and axillary dissection because the lesion was misdiagnosed as a tubular carcinoma or an adenosquamos carcinoma.3,4 However, tubular carcinoma rarely involves the nipple. Histologically, tumour cells of tubular carcinoma often exhibit apical cytoplasmatic snouts and are often associated with micropapillary or crybriform types of low-grade ductal carcinoma in situ and/or flat epithelial atypia. The basement membrane and myoepithelial cells around neoplastic tubules are absent, which can be confirmed by immunohistochemical stain for p63 and/or smooth muscle myosin heavy chain, in difficult cases. The presence of squamous differentiation is another distinctive feature not observed in tubular carcinomas. 2 The differential diagnosis from low-grade adenosquamous carcinoma is not so clearly defined. Low-grade adenosquamous carcinoma is a welldifferentiated tumour with both glandular and squamous differentiation. Although the histological appearance is similar to infiltrative syringomatous adenoma, more peripheral localization in the breast parenchyma and ability to metastasize are two features that characterize low-grade adenosquamous carcinoma. In contrast, infiltrating syringomatous adenoma of the nipple is benign, but locally expansive lesion, with the ability to infiltrate smooth muscle and nerve but not to metastasize. 5 It has a tendency for local recurrence as a result of an incomplete excision. 5 However, a single case of infiltrating syringomatous adenoma with micrometastasis to a sentinel lymph node was reported. 6 Due to localization in differential diagnostic consideration, nipple adenoma should also be included. The main difference is that nipple adenoma often occurs with the necrosis or erosion of the epidermis, and usually exhibits florid ductal hyperplasia, with or without a mild degree of cytological atypia.
Conclusion
Infiltrating syringomatous adenoma is a rare lesion and deserves special attention to avoid misdiagnosis as a malignant process with subsequent unnecessary treatment. Because of simultaneous bilateral occurrence of this entity presented in this report, we believe that finding of infiltrating syringomatous adenoma in one breast should prompt careful examination of the opposite breast with adequate follow-up.
Learning points
Infiltrating syringomatous breast adenoma is a rare, benign, infiltrating neoplasm of eccrine origin located in the dermis of the areola and nipple;
Tumour is composed of angulated glandular structures lined by an inner layer of epithelial cells and by an outer layer of myoepithelial cells immersed in desmoplastic stroma;
Squamous differentiation of the luminal cells with keratin cyst formation is frequently observed;
Perineural growth may be seen and is not indicative of malignancy;
Finding of infiltrating syringomatous adenoma in one breast should prompt careful examination of the opposite breast.