
Abstract
Endovascular repair of abdominal aortic aneurysm is a common procedure and not without complications. The aim of this study was to evaluate the early results of the Anaconda endograft (Vascutek Ltd., Inchinnan, Scotland, UK) in 106 patients in three hospitals in the west of Scotland. A prospective registry of 106 consecutive patients undergoing endoluminal repair of their abdominal aortic aneurysms using the Anaconda device was set up to record the clinical outcomes, with a mean follow-up of two years. There was no 30-day perioperative mortality in the 106 patients. Only type II endoleaks were detected on serial computed tomography scanning at follow-up. Technical success was achieved in 99% (105/106) in this study; one patient was converted to open surgical repair. Two cases of proximal device migration (>1 cm) were detected at one month and 19 months, respectively, with no associated endoleak or sac enlargement. Five cases of endograft limb thrombosis were noted in this study. Our early clinical experience with the Anaconda endograft compares favourably with other commercially available endografts in the treatment of abdominal aortic aneurysms. The main advantages of this device are that it is re-deployable and that it has a magnetic wire system which makes it easy to implant.
Introduction
Endovascular repair of abdominal aortic aneurysm has become a routine operation in the UK since it was shown in randomized studies to reduce the perioperative mortality when compared with open surgery.1–3 While initially patients with ideal anatomy in the proximal aortic neck and distal landing zones were selected for endoluminal treatment, with experience more challenging cases have been treated successfully. In gaining exclusion of the abdominal aortic aneurysm it is important for the endoluminal device to achieve proximal seal without compromising the renal arteries.
The Anaconda device (Vascutek Ltd., Inchinnan, Scotland, UK) is manufactured with a thin woven Dacron fabric over a nitinol stent skeleton. Two nitinol hoops create a proximal seal; with four sets of pins to prevent distal migration. Underneath the two hoops and pins, there is a portion of the device which is not supported by stents. Radio-opaque markers locate the correct orientation of the device within the aneurysm sac at implantation. Further radio-opaque markers define the contralateral gate and the correct alignment of the contralateral limb. The delivery sheath is attached to the endograft by two threads connected to a control system which allows the device to be re-deployed within the proximal aortic neck at implantation. During the study, the Blue Glide delivery sheath (Vascutek Ltd.) was introduced, which has a hydrophilic coating to assist implantation of the device through diseased and tortuous iliac arteries. A magnetic wire system helps the operator to gain rapid cannulation through the contralateral gate.
The aim of this study was to evaluate our initial clinical experience with the Anaconda endoluminal graft in the treatment of patients with abdominal aortic aneurysm.
Methods
A total of 106 consecutive patients undergoing abdominal aortic aneurysm using the Anaconda device were entered in to a prospective registry between June 2005 and September 2009. The patient demographic and risk factors are shown in Table 1.
Patient demographic and risk factors
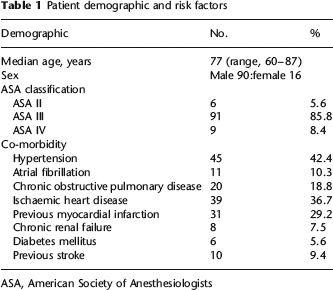
ASA, American Society of Anesthesiologists
Preoperatively a contrast-enhanced multislice computed tomography (CT) scan was performed to assess the anatomy of the proximal and distal landing zones and the suitability for endovascular repair. Some patients also underwent preoperative measuring catheter aortography or intravascular ultrasound. 4 Cases were routinely discussed at the local multidisciplinary vascular meeting prior to performing endovascular aneurysm repair (EVAR).
The inclusion criteria for treatment were infrarenal abdominal aortic aneurysms with a neck length of ≥15 mm and a proximal neck diameter of ≤31.5 mm. The common iliac arteries needed to be approximately 7 mm in diameter in order to accommodate the 24F delivery system. Exclusion criteria were suprarenal aneurysms, short proximal neck length and larger neck diameters of more than 31.5 mm as well as excessively narrow or diseased iliac arteries.
Procedure
Both femoral arteries were exposed and controlled surgically using either general or regional anaesthesia. Routinely, a pigtail angiographic catheter was advanced to a level proximal to the renal arteries using a retrograde femoral approach from the contralateral side. The Anaconda device was introduced over a stiff 0.035-inch guidewire into the proximal aortic neck. An aortogram was then performed using the pigtail catheter to create a ‘road map’. The endoluminal graft was deployed by pulling the delivery sheath back. An assessment was then made of the position of the device and its ability to gain a proximal seal together with its relation to the renal arteries. In most cases the ‘peaks’ of the device were positioned at the level of the renal arteries and the ‘valleys’ a few millimetres below the renal arteries. If initial deployment was not satisfactory, then the device was partially re-captured using the control system and its position adjusted. Two contralateral radio-opaque markers demonstrated that the device was oriented correctly within the aneurysm sac.
After marking the position of the hypogastric arteries with arteriography, a magnet wire (Vascutek Ltd.) was introduced using an 8F sheath from the contralateral femoral artery. The magnet on the contralateral wire was manipulated to attract and link with another magnet on the main delivery system (Supplementary Figure 1). When these two magnets were attached and bonded together, they were then advanced through the contralateral gate by introducing both magnet wires together. This gained contralateral wire access. The Anaconda extension limbs were then deployed, taking care to avoid compromising the hypogastric arteries. While the main body of the device could still be re-positioned even after implantation of a contralateral limb, once the threads connecting to the control system were removed, the device was completely released and fully deployed. Completion aortography was used to confirm seal and patency. All of the procedures were performed in an operating theatre using a mobile intensifier or in a radiology endovascular suite. Additional procedures such as embolization of the hypogastric vessels were generally performed as separate procedures prior to endovascular repair. All patients received antibiotic prophylaxis and intravenous heparin. The Anaconda device was deployed and implanted in two hospitals by interventional vascular radiologists and in a third hospital by two vascular surgeons. All 106 consecutive patients were entered into the registry. A contrast-enhanced CT scan and abdominal X-ray were routinely performed just before discharge, one month, six months, 12 months and annually thereafter. All patients were discharged on best medical therapy, which generally included an antiplatelet and lipid-lowering drug. All patients were followed up clinically. All deaths during patient follow-up were identified through the Scottish Death Registry 5 and CHI 23 National Health Service (NHS) website 6 which provided information on the cause of death.
Results
A total of 106 patients underwent EVAR using the Anaconda stent graft system. There were 90 men and the mean age was 77 years (range, 60–87 years). The mean neck length was 2.5 cm (range, 0.7–4.5 cm) and the mean aneurysm diameter was 6.3 cm (range, 4.8–10.7 cm). Ten cases were performed with an aortic aneurysm diameter less than 5.5 cm (range, 4.8–5.4 cm), either for expanding or symptomatic aneurysms. Associated iliac disease was present in 27 patients (severe tortuosity, 5; aneurysm, 10; and occlusive disease, 12). Of 10 cases with concurrent iliac aneurysms, six were treated by embolization of the hypogastric arteries. All 12 cases with iliac occlusive disease were treated by preliminary balloon angioplasty (see Table 2). Two cases required proximal extension cuffs in order to obtain seal at the time of implantation.
Morphology of aneurysms and pre-EVAR procedures during EVAR

AAA, abdominal aortic aneurysm
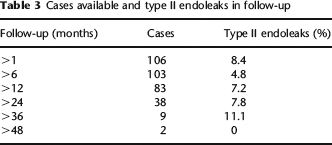
There was no 30-day perioperative mortality in the 106 cases. Ten patients died during subsequent follow-up: all of these deaths were non-aneurysm related. Type II endoleaks were detected at one, six, 12, 24, 36 and 48 months in 8.4%, 4.8%, 7.2%, 7.8%, 11.1% and 0% of patients, respectively (Table 3). There were no type I, III or IV endoleaks. Technical success was achieved in 99% (105/106) in this study. Only one patient was converted to open surgical repair of the aortic aneurysm because of loss of wire access.
Cases available and type II endoleaks in follow-up
The systemic and local complications are listed in Table 4. One patient who had a significant history of cardiac disease subsequently developed unstable angina. He was successfully treated by an emergency coronary artery bypass graft operation.
Systemic and local complications
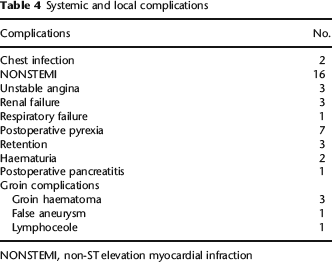
NONSTEMI, non-ST elevation myocardial infraction
Device-related complications are shown in Table 5. One patient developed acute aortic rupture of the proximal aortic neck following ballooning to treat a perioperative type I endoleak. This was immediately detected and a proximal extension cuff was placed just under the level of renal arteries. However, both renal arteries were compromised without causing occlusion; despite this the patient developed renal failure requiring subsequent dialysis. Renal artery impingement by the device was noticed in another case after one-month follow-up due to a proximal migration of the device, without a change in the renal function.
EVAR-related complications

AAA, abdominal aortic aneurysm
Five cases of endograft limb thrombosis were noticed in follow-up. Four of these were treated by femoro-femoral crossover grafting without any further complications in the follow-up. One other patient who developed subsequent limb thrombosis one year postoperatively did not require any further intervention. All of the patients with endograft limb thrombosis had significant iliac artery disease noted on their preoperative investigations. Hypogastric artery occlusion was detected in three other patients at follow-up CT scanning. The occlusions were bilateral in one case and unilateral in two. All three patients remained asymptomatic with no further intervention required.
Discussion
The early clinical results in this cohort of patients compare favourably with published series of other commercially available endografts.7–9
The long-term follow-up data from the EVAR I trial have recently been published 10 and the first graft-related complications were related as type I endoleaks (9.9%), type II endoleaks (19.7%), type III endoleaks (2%), graft migration (7.6%) and graft thrombosis (6.5%). Compared with these data, our results using the Anaconda device represent a far more favourable outcome. It is to be noted, however, that the devices used in the EVAR 1 trail were principally second- and third-generation endografts.
There was no 30-day perioperative mortality in our cases and no aneurysm-related death in the follow-up. Together with the relatively low endoleak rate11–14 in our series, this indicates that the Anaconda device is both safe and effective. We have found that the ability to re-deploy the device in the proximal neck is useful. Indeed, even when initial deployment appears satisfactory, we have tended to make minor adjustments to the position of the device. While this ability to re-position the device should protect the renal arteries from occlusion, one patient in this series developed renal failure requiring dialysis. This was caused by having to deploy a proximal cuff urgently in order to treat an acute rupture of the aorta just underneath the renal arteries. Another patient was also noticed to have a renal artery occlusion at one month postoperatively. The device had migrated proximally in a short neck, more than 1 cm from its initial position. Fortunately, this patient continued to have normal renal function and remained asymptomatic. The ‘valley’ of the proximal hoops underneath the renal arteries can rise proximally following implantation, and care needs to be taken to position the endograft a few millimetres distal to the lowest renal artery.
Another potential advantage of the Anaconda device is that the Dacron is unsupported by any stent for 4 cm distal to the two nitinol hoops. This means that the device can conform to the anatomy of an angulated neck (Supplementary Figure 2).
In practice, we have found the magnet wire system to be an extremely helpful and rapid way of gaining contralateral access and implanting the contralateral limb. Connecting the two magnets generally takes no more than a couple of minutes. However, in large aneurysm sacs it can take longer. Two different magnetic wires are available: one flexible, the other stiff. In two patients we had to resort to a brachial access route in order to cannulate the contralateral limb.
Conclusion
In summary, we have enjoyed the benefits of the design features of the Anaconda device, particularly its ability to be re-deployed in the proximal aortic neck after initial implantation. The two nitinol hoops are able to provide good proximal seal even in diseased aortic necks, and the magnetic wire system provides rapid contralateral wire access.
Supplementary material
The supplementary material accompanying this article can be found online at: http://smj.rsmjournals.com.
Footnotes
Acknowledgements
The authors would like to thank A J McKay, P N Rogers, D Bryne and D Kingsmore of Gartnavel General Hospital, Glasgow; George Welch, Wesley Stuart and D Bain of Southern General Hospital, Glasgow; and Sam Miller of Hairmyres Hospital, East Kilbride.