
Abstract
The views of the parents of children undergoing elective surgery are not well represented in the literature. The aim of this study was to identify the priorities of parents with a view to improve their satisfaction. A questionnaire-based survey was conducted among parents of children undergoing elective surgery between November 2007 and March 2008. A total of 337 completed questionnaires were received. A similar survey was conducted among 12 surgeons, and their views were compared. Forty-three percent of parents preferred to know about a procedure on the day of surgery while others wanted the information in advance. Parents were most concerned with the complications of surgery and least concerned with the scar. Most of the surgeons thought it was not essential to mention their level of experience and the detailed surgical procedure to the parents while obtaining consent for surgery. In contrast, the parents thought that knowing the experience of the operating surgeon and the detailed surgical procedure was more important than knowing the duration of operation and the surgical incision. Face-to-face discussion with a surgeon was the most preferred mode of communication. Although 82% of parents have access to the Internet, booklets were more popular among parents than online information. Twelve percent of parents wanted the information in a foreign language. This survey reveals the perspective of parents about their child's surgery and identifies the differences in opinion between patients and surgeons about the information to be provided before surgery. Tailoring information to the parents’ priorities will improve parent satisfaction.
Introduction
The Department of Health guidance on informed consent states that children and their parents clearly need enough information before they can decide whether to consent to, or refuse, treatment. In particular, they need information about the benefits and the risks of the proposed treatment, what the treatment will involve, what the implications of not having the treatment are, what alternatives may be available and what the practical effects on their lives of having, or not having, the treatment will be.1,2 It is essential that medical information should be provided in a form that the particular parent can understand. It may also involve the use of interpreters in cases in which the first language of the child or the parents is not English.1,2
It is recommended to use up-to-date written material, visual and other aids to explain complex aspects of the investigation, diagnosis or treatment. 2 In addition to a consultation, providing more tailored information, for example, a standardized written document (information booklets), improves the decision-making process involved in giving informed consent.3,4 However, these information booklets are not widely available in different languages.
More than 60% of households in Great Britain had Internet access. 5 Due to increased availability the Internet is becoming an important educational tool for the parents. Most of the parents who accessed the Internet for medical information found it to be useful, but some found that there was too much information and that it was too technical. 6
Significant differences in priorities of patients and medical professionals have been previously identified.7–9 The aim of this survey was to identify information that is important to parents and to direct the paediatric surgeons to focus on these elements.
Methods
Following approval from the Department of Clinical Governance, the parents of all 464 children undergoing elective surgery from November 2007 to March 2008 at a tertiary paediatric surgery centre were requested to participate. The participation was voluntary and anonymous, and parents were told that their refusal to participate in the study would not impact on treatment.
A standardized 10 one-page tick-box questionnaire (Supplementary Figure 1) was developed by the authors using information from guideline documents published by the Department of Health 1 and a previously published study 8 that showed those aspects of surgery considered to be most important by the patients. The questionnaire was independently reviewed and accepted by all paediatric surgical consultants before implementation.
The questionnaires were handed over to parents from the Paediatric Admissions Office once the decision for surgery was made after consultation with a surgeon. At this stage the parents already had the opportunity to discuss the operation with the surgeon and their questions were answered. Parents were asked to return the forms either by post (prepaid envelopes were provided) or to bring them on the day of the operation. Where the parents required interpreters, it was advised that they answer the questions with the interpreters or any friend or family member who understands English.
Twelve paediatric surgeons were asked to answer some of the relevant questions from the previous questionnaire on a modified questionnaire (Supplementary Figure 2). Responses from parents and surgeons were compared.
Completed questionnaires were collected and data were entered onto a database for analysis. SPSS v17.0 (SPSS Inc., Chicago, IL, USA) was used for data analysis and Fisher's exact test was used to analyse categorical data.
Results
A total of 337 (73%) completed questionnaires were received from the parents. Forty-three percent (n = 133) parents preferred to know about the procedure on the day of operation, but 57% (n = 177) wanted the information earlier. Of those surveyed, 82% had access to the Internet. The Internet was more widely available to English-speaking population (84%) compared with non-English-speaking population (74%), but this difference was not statistically significant (P = 0.1699). Most parents (86%) wanted to speak to the surgeon and know about the procedure. Of the other forms of communication, booklets (12%) were more popular to parents than the Internet (2%). As this question was to identify the most preferred form of communication, answers with multiple responses were excluded from analysis. Eleven percent (n = 38) requested communication in a foreign language.
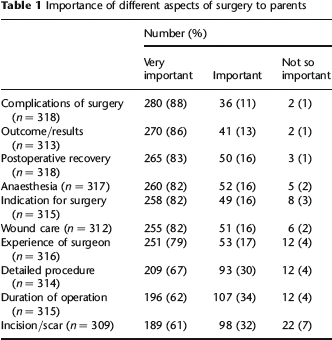
Table 1 shows how the parents graded different aspects of surgery according to the importance for them to know them before surgery. For 88% (n = 296) of parents, to know the complications of surgery was ‘very important’, but to know about the scar was ‘very important’ for only 61% (n = 205) of parents.
Importance of different aspects of surgery to parents
All 12 paediatric surgeons who were approached participated in the survey. All surgeons felt that mentioning all aspects of surgery was very important while obtaining consent except for ‘experience of surgeon’ and ‘detailed surgical procedure’. To 67% of surgeons it is ‘not so important’ to mention the detailed surgical procedure to the parents. None of the surgeons thought it was ‘very important’ to disclose their level of experience in the particular procedure unless specifically asked by the parents (Table 2).
Importance of different aspects of surgery to surgeons

The opinions of surgeons were significantly different from those of the patients regarding experience of surgeon (P < 0.0001), detailed surgical procedure (P = 0.0001), duration of operation (P = 0.0181) and surgical incision/scar (P = 0.0154) (Table 3). Even after adding up ‘very important’ and ‘important’ responses, the difference remained significant for experience of surgeon (P = 0.0015) and detailed surgical procedure (P < 0.0001).
Comparison of priorities of parents and surgeons
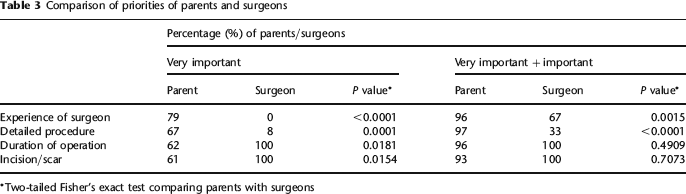
Two-tailed Fisher's exact test comparing parents with surgeons
Most of the parents were satisfied with the present information delivery system. Only 3% (n = 10) of parents found it unsatisfactory. Compared with English-speaking parents, fewer non-English-speaking parents found the doctor–patient communication excellent (P = 0.0082) and a higher proportion of them found it unsatisfactory (Table 4).
Parent satisfaction with the present system of communication
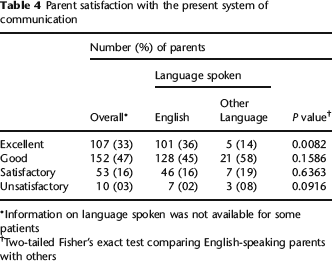
Information on language spoken was not available for some patients
Two-tailed Fisher's exact test comparing English-speaking parents with others
Discussion
It has been previously demonstrated that for all components of informed consent, both parents and children recalled fewer items than they had been told by the surgeon just 15–30 minutes earlier. 11 Although it has been shown that patients who were given written information have better understanding and postoperative recall of information, most parents prefer to speak to a surgeon to know about a procedure.12–14 Several previous studies were undertaken to identify the views of patients, aiming to provide tailored information to them, but none of them were done involving parents in a paediatric surgical setting.7–9,15
It was observed that almost half (45%) of parents would prefer to know about the surgery on the day of operation and not in advance. Keeping this in mind, the paediatric surgeons should explain the surgery to parents well in advance and reiterate again on the day of surgery.
In our study, we found face-to-face discussion with the surgeon was the most preferred method of communication for parents. This was similar to the findings of a previous study. 6 It is expected that parents would prefer to speak to the surgeon to know about the surgery, but in this survey 14% of parents preferred booklet/Internet to face-to-face discussion with the surgeon. This signifies the importance of available written materials and online references for paediatric surgical procedures.
Paediatric surgery involves a wide range of complex surgical procedures and written information about different operations are not widely available. The website of the British Association of Paediatric Surgeons has downloadable patient information for only six procedures. The introduction of procedure-specific consent forms was considered to be a solution to this problem, but a national survey showed that they are not very popular among paediatric surgeons, probably due to paucity of studies regarding them. 16
Internet access among parents in this study was higher (82%) than the national average. 5 Previous studies showed that 32–53% of parents accessed the Internet for health information; however, in this study, only 1.5% of parents preferred to receive information via the Internet.6,17 As a result of the survey, our team has written patient information sheets for common paediatric surgical procedures in order to make written information easily available to parents. This information is available for parents from the hospital website. There is no official source giving a detailed breakdown of how many people in the UK do not speak English and the different languages spoken in the UK. A significant number of parents (11%) preferred communication in a foreign language. Translation and interpretation services are available in the National Health Service (NHS) for all languages spoken by parents in this study. 18 Nineteen percent (n = 7) of parents who preferred booklets as the most preferred mode of communication also required the information in a foreign language. Patient information booklets were not available in foreign languages in our centre and there were no studies looking at the quality of health information available in foreign languages on the Internet. However, electronic information booklets could easily be translated using translation software and websites.
There are disparities between the priorities of patients and surgeons regarding the importance of different aspects of informed consent, a fact that has been shown in previous studies.7–9,15 Complications, outcome/results and recovery after surgery were considered ‘very important’ by most parents (Table 2). These findings are similar to previous studies.8,15 Few parents thought scarring and duration of surgery were ‘very important’. Most of the surgeons thought it was not essential to mention to the parents their level of experience and the procedure in detail. Seventy-nine percent of parents thought it was ‘very important’ to know the level of experience of the surgeon and 67% of them thought it was ‘very important’ to know about the detailed procedure. We recommend that, in order to meet the expectations of the parents, all surgeons should disclose their level of experience and explain the surgical procedure in detail while obtaining consent for surgery.
While designing the questionnaire, our team of investigators expected that all parents would consider all 10 aspects of surgery to be ‘very important’. It was unexpected to find that only 61% of parents thought it was ‘very important’ to know about the scar and 7% of parents thought it was even not important. Our survey can be criticized for using a grading system (very important, important and not so important) instead of a visual analogue scale, but this was an attempt to keep the questionnaire simple for parents. The results are arranged in order of ‘very important’ responses. There may be an argument that ‘very important’ and ‘important’ do not differ a lot; however, it can be assumed that parents who chose ‘important’ despite having the option to choose ‘very important’ should have considered that aspect of surgery less concerning to them.
Conclusion
Good patient communication is an integral part of modern medical practice. 19 The amount of medical information given to parents before surgery may be difficult for them to comprehend and remember. Tailoring the information delivery according to the priorities of the parents is likely to improve understanding and overall satisfaction.
We recommend that an experienced surgeon discuss the procedure with the parents well in advance and place emphasis on the information that parents really want to know. Supplementary written materials should be made available with translations where needed.
Supplementary material
The supplementary material accompanying this article can be found online at: http://smj.rsmjournals.com.