
Abstract
The General Medical Council emphasizes the cultivation of professional behaviours among medical students from early undergraduate years. Learning professional behaviours, however, is a progression and is constituted of several developmental stages. Behaving with academic integrity may be the first stage. In an educational setting, academic integrity is represented by a collection of diverse behaviours. Although there is consensus within the medical community that the absence of (or lapses in) academic integrity is unacceptable, the level of sanctions recommended for medical students is controversial. In the main, these punitive decisions over students are taken by teachers and clinicians. What sanctions would students suggest for a colleague who is academically unprofessional? This study reports the sanctions recommended by 375/700 (54%) of the students of one Scottish medical school in relation to lapses in academic integrity.
Introduction
Despite the proliferation of studies relating to professionalism, teaching and learning among undergraduate medical students, there are little data to guide the determination of standards and appropriate sanctions for lapses.1,2 Van Mook et al. 3 have pointed out that:
Opinions vary and evolve about how students and professionals should behave. Medical students are nevertheless expected to demonstrate the currently professionally appropriate and ethical behaviour. Knowing what constitutes this behaviour however, appears to be extremely challenging for students as well as teachers, since context (e.g. time, place and culture) all influence the expected behaviour.
Researchers4,5 who have tried to develop scenarios relating to professional dilemmas have found it very difficult to agree appropriate responses among ‘expert’ panels, and they are highly culturally specific. 6 Our goal was to determine a set of agreed sanctions at various levels of medical education and training to guide the development of a consistent approach across UK medical schools.
Methods
We identified approximately 100 unprofessional behaviours related to lack of academic integrity at the initial stage of undergraduate education in a literature review of more than 30 studies of issues related to academic integrity in undergraduate medical and health professions courses. With the assistance of two research assistants, these were reduced after duplications were removed and consolidations were made to 41 items (Table 1).
The survey asks you to rate your responses to the following 41 statements

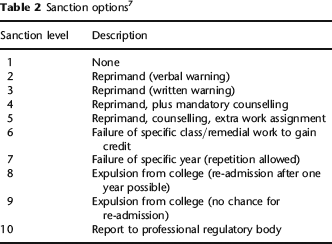
Following Teplitsky 7 respondents were asked to recommend appropriate sanctions for a one-time infraction with no mitigating circumstances. In addition to Teplitsky's nine sanctions, we added a tenth, report to the professional regulator, i.e. the General Medical Council (Table 2).
Sanction options 7
The inventory was developed as a Bristol Online Survey. Permission to administer it to the student population at a Scottish medical school was given by the university's research ethics committee. The Head of the Division and the Dean of the Medical School supported the project, and the Secretary of the Medical School issued it through his office to the approximately 700 medical school students (some of whom were on attachments out of the school and not accessing their email). All respondents were anonymized. Two email reminders were sent to all students at two- and four-week intervals before the closure of the survey after six weeks (Table 3).
Median sanctions proposed for each unprofessional behaviour

Results
Of the 700 medical students, 375 responded: a response rate of 54%. Forty-two (11%) were first-year students; 82 (22%) second-year; 75 (20%) third-year; 74 (20%) fourth-year; and 102 (27%) fifth-year students. The male-to-female ratio was 1:2, which was typical of the full cohort. A majority (259; 69%) of respondents were in the 20–24 years age group; 66 (18%) were younger than 20 years and 49 (13%) were older than 25 years.
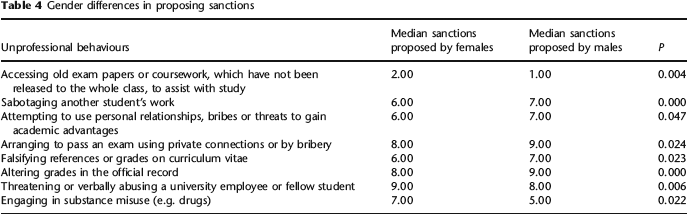
There were several statistically significant gender differences in the recommended sanction as set out in Table 4, but they were not all in one direction.
Gender differences in proposing sanctions
There was little difference by age group in the recommended sanctions. However, failing infection control procedures was proposed with stricter sanction by 17–19 age group than by their older counterparts (P = <0.05).
There were several statistically significant differences in the sanctions between the different year groups as shown in Table 5, but there were only two differences of more than one point. The junior years recommended a sanction of 5 (reprimand, counselling, extra work assignment) for ‘intentionally falsifying test results or treatment records in order to disguise mistakes’, whereas the fourth-year respondents proposed sanction 7 (failure of specific year [repetition allowed]) while fifth-year respondents proposed sanction level 6 (failure of specific class/remedial work to gain credit). This result may alert the medical school to a need for clear guidance, especially in the junior years and at the point at which students move into more direct clinical work.
Variation of sanctions with the year of study
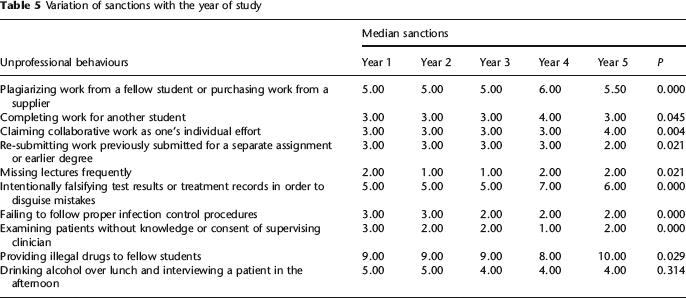
Interestingly, the fourth years recommended that ‘examining patients without the knowledge or consent or supervising clinician’ should be ignored, while the other years gave it a relatively low sanction. Here again guidance might be required to clarify this issue as students move into more direct clinical contact with patients.
Discussion
The UK Council for Healthcare Regulatory Excellence in its July 2009 Annual Report called for ‘greater consistency to fitness to practice procedures across UK medical schools’ and the evolution of a ‘common sanction set’ across the health professions. The UK General Medical Council now requires proof of fitness to practice before a graduate can provisionally register as a doctor. Medical schools are expected to have fitness to practice procedures in place. Medical Students: Professional Behaviour and Fitness to Practise was published in 2007. This paper reports a study of medical students’ recommended sanctions for first time offences of poor professionalism with no mitigating circumstances as part of a wider study to benchmark appropriate sanctions for use in UK medical schools and beyond. 8