
Abstract
The aim of this study was to study the effects of rosuvastatin in patients with rheumatoid arthritis (RA) looking at the C-reactive protein (CRP), interleukin-6 (IL-6) and joint disease activity. Fifty RA patients were randomized in a double-blind placebo-controlled trial to receive either 10 mg of rosuvastatin or placebo as an adjunct to existing disease-modifying antirheumatic therapy. Patients were followed up for a six-month period. Measurements were done at baseline and six months. CRP and IL-6 were measured in the blood. RA disease activity was measured using disease activity score based on 28 joint counts (DAS 28). When analysing from baseline to six months there was no difference between the rosuvastatin and placebo groups in rheumatoid disease activity (–0.01; standard deviation [SD], 1.08; and +0.18; SD, 0.95; respectively; P value 0.509). There was a trend towards improvement in CRP in the rosuvastatin group (–3.23; SD, 18.18) compared with the placebo group (+17.43; SD, 38.03); P value, 0.161. IL-6 showed a trend towards worsening in the rosuvastatin group (+0.15; SD, 1.09) compared with placebo (–0.73; SD, 1.4); P value, 0.054. These data show that rosuvastatin with might decrease the CRP independent to IL-6 in patients with RA but does not improve the overall rheumatoid disease activity.
Introduction
The lifespan of patients with rheumatoid arthritis (RA) is shortened by approximately 15–20%1,2 from the date of onset of the illness. Between 34% and 40%1,3 of the excess deaths are from cardiovascular (CV) causes. HMG-CoA (3-hydroxy-3-methylglutaryl coenzyme A) reductase inhibitors (statins) reduce CV morbidity and mortality. Mevalonate is the precursor not only of cholesterol but also of many other non-steroidal isoprenoid products. Inhibiting the HMG-CoA reductase will decrease both the cholesterol and these isoprenoid products which affect various cellular functions. Both lipophilic and hydrophilic statins like rosuvastatin has been shown to have some anti-inflammatory effects. Statins are also potent immunomodulators as evidenced by the animal experiments where statins selectively blocked leukocyte function antigen-1-mediated adhesion 4 and monocyte chemotactic protein-1 expression. 5 It is not known whether such effects on laboratory can be translated to clinical practice. RA is a prototypical systemic inflammatory disease and we wanted to find out whether rosuavastatin can have any clinically useful effect on inflammation and joint disease activity in our Tayside population. We therefore conducted a pilot randomized double-blind placebo-controlled trial to test the effects of rosuvastatin in patients with RA.
Methods
This study was approved by the Tayside Research Ethics committee and sponsored by the University of Dundee. We aimed at recruiting 50 patients from rheumatology clinics throughout Tayside in Scotland. Patients were selected from a high-risk population of hospital clinic attendees, defined as RA ≥5 years disease duration, and all of them were RA latex seropositive or immunoglobulin M (IgM) rheumatoid factor (RF) enzyme-linked immunosorbent assay (ELISA) >14 IU/mL. The participants were of either sex and ≥40 years of age. Patients should have either a C-reative protein (CRP) ≥10 mg/L, erythrocyte sedimentation rate ≥25 mm/h or plasma viscosity ≥1.78. Patients should be on stable disease-modifying antirheumatic drug (DMARD) for at least three months. Patients on cyclosporine, hormone replacement therapy or other medications known to be contraindicated with this form of drug were excluded. The patient's hospital records were scrutinized for evidence of symptomatic vascular disease. Any patient not free from vascular disease symptoms was excluded. In addition, the exclusion criteria consist also of those already taking lipid-lowering therapy, known diabetes, significant renal disease (glomerular filtration rate ≤30), untreated hypothyroidism, alcohol intake ≥21 units/week, elevated aspartate transaminase or alanine transaminase or creatine kinase. Also excluded were the subjects with a total cholesterol level of ≥7.5 mmol/L as it might be argued that such patients merit primary prevention on the basis of dyslipidaemia alone.
Informed consent was obtained from all 50 patients. All treatment changes during the study period were recorded. Patients were randomly allocated either rosuvastatin (crestor) 10 mg or placebo. The drugs (rosuvastatin and placebo) were provided by Astra Zeneca Ltd. (London, UK). Computerized randomization was done by an independent person from Tayside pharmacy and both patients and doctors were unaware of drug allocation. In order to blind the trial drugs during the study period, the blood tests for cholesterol were checked by a research nurse who was not involved in the clinical assessment of patients. The outcome measures were CRP, interleukin-6 (IL-6), joint disease activity score (DAS 28) and Health Assessment Questionnaire (HAQ), which is a validated functional measure in RA patients. We also measured the lipid profile at baseline and at six months.
After screening, study visits were scheduled for 0 and six months. We did safety blood tests for creatine kinase, liver function and renal function during both visits; an additional safety test at three months was also done as recommended by the summary of product characteristics for rosuvastatin. Any change in the treatment and adverse events were recorded throughout the study period.
We prepared plasma and serum samples immediately after venepuncture. Lipid profile and safety blood tests were done straightaway and the remainder was stored at –70°C until assay. A highly sensitive CRP assay using ELISA was used. The flow cytometric analysis was used to measure IL-6 (Human Cardiovascular; Bender Medsystems, Vienna, Austria).
RA disease activity was measured using DAS 28 score, a validated composite RA disease activity score,6,7 which was calculated as previously described. 7 We also recorded Modified Stanford HAQ.
Statistical analysis
As this was a pilot trial the power could not be calculated. Fifty patients were randomly selected in Tayside rheumatology clinics. Two patients dropped out of the study just before their baseline visit but after randomization, so only 48 patients were analysed. We accounted for dropouts by carrying their baseline value forward to six months (i.e. no change assumed). Baseline data are summarized as mean (standard deviation [SD]) for continuous variables and number of patients (%) for categorical variables. The P value for baseline variables was obtained using independent sample t-test. The outcomes at six months were analysed using univariate analysis of variance adjusting for potential confounders. The differences between baseline and six months were analysed using independent sample t-test. A P value <0.05 was considered to be statistically significant. All the analysis were done using SPSS version 15 (SPSS Inc., Chicago, IL, USA).
Results
A total of 174 patients assessed for eligibility of which 50 were randomized to receive either 10 mg of rosuvastatin or placebo (Supplementary Figure 1). Both groups were generally comparable (Table 1). There was a slight trend towards the placebo group havingmore tender joints and rheumatoid disease activity, though it was not statistically significant. More patients allocated placebos were on methotrexate and more allocated rosuvastatin were on sulfasalazine (Table 2). The usage of combination DMARDS and antitumour necrosis factor (TNF) therapies was also comparable between both groups (Table 2). Frequency of steroid usage in the study population is shown in Table 3, which was not very different between the groups. There were three patients in each group requiring top-up steroids for RA flare.
Baseline characteristics
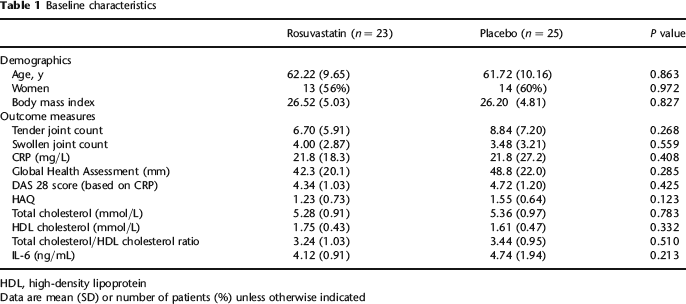
HDL, high-density lipoprotein
Data are mean (SD) or number of patients (%) unless otherwise indicated
DMARD Therapy
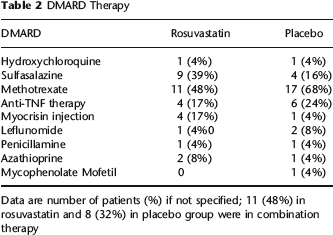
Data are number of patients (%) if not specified; 11 (48%) in rosuvastatin and 8 (32%) in placebo group were in combination therapy
Steroid usage
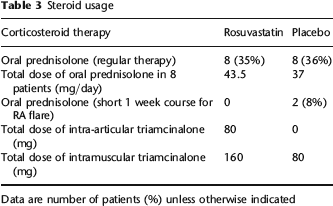
Data are number of patients (%) unless otherwise indicated
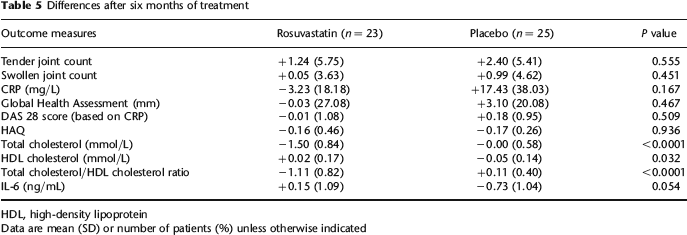
Table 4 documents the outcomes for each study arm at the end of study (6 months) analysed by univariate analysis of variance. Table 5 documents the differences from baseline to six months. There is a trend towards improvement in CRP and worsening in IL-6, which is more obvious in the graph obtained by univariate analysis (Supplementary Figures 2 and 3) when analysed using univariate analysis of variance. DAS 28 and the individual components of it did not show any significant difference between the two groups.
Outcome after six months of treatment
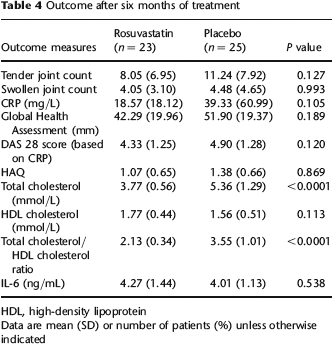
HDL, high-density lipoprotein
Data are mean (SD) or number of patients (%) unless otherwise indicated
Differences after six months of treatment
HDL, high-density lipoprotein
Data are mean (SD) or number of patients (%) unless otherwise indicated
Adverse events
There were three serious adverse events in two patients. One was a patient with elevated alanine transaminase (more than twice the upper limit) who was taking rosuvastatin; it was normalized after stopping the study drug. The same patient also had a hospital admission for slightly displaced hip joint prosthesis that was operated on. The third serious adverse event was also a hospital admission in a patient on placebo for osteomyelitis of the feet. This patient, however, continued taking the study drug throughout the study period. Events leading to withdrawal are shown in Supplementary Figure 1. In general, rosuvastatin was well tolerated in the study population.
Discussion
We have shown that rosuvastatin does not improve the rheumatoid disease activity despite the trend towards improvement in CRP. This suggests that the relatively minor effects on CRP have no clinical relevance in improving the overall inflammatory burden of this condition. IL-6 usually correlates well with CRP as it stimulates the synthesis of CRP from the liver. 8 In our study we notice that the effects of rosuvastatin on IL-6 to be the opposite of CRP, suggesting that rosuvastatin might have some direct effects on the liver to alter the CRP secretion/synthesis. The effects on CRP did not reach statistical significance, which we believe could be due to wider confidence intervals. RA is a fluctuant disease with intermittent flares that fluctuates the CRP to a large extent; it could explain the wider confidence intervals we observed in our group. The P value for IL-6 nearly reached statistical significance (0.054), so it is probable that inflammation in the rosuvastatin group did get slightly worse. However, it is offset in DAS 28 calculation by the fall in CRP. Our trial was conducted in high standards, so it is impossible that this lack of effect on rheumatoid disease activity could just be due to chance. It is possible that higher doses of rosuvastatin could have shown the significant difference in the outcome markers, but in a patient group like ours who are already on lots of tablets such as DMARDS and analgesics, it would be norm to start them on 10 mg of rosuvastatin. It is also possible that more number of patients in our study could have increased the power to show a significant difference in the trends we observed but we could not have predicted this before starting the study. However, this study clearly shows that apart from CRP, other individual components of DAS 28 do not show any trend towards improvement. We could not say based on this study whether the effects on CRP is independent of cholesterol-lowering effect.
Our study group is more of real-life patients where RA disease activity is targeted aggressively by combination therapy and anti-TNFs but still has some residual inflammation and an adjunctive treatment is necessary to control it. Nearly 40% of our patient group was on combination DMARDs and 20% of them were on anti-TNF therapy.
We do recognize important limitations in our study. The design chosen offers advantages in facilitating singlecentre recruitment over a short period. This study was done primarily as a proof of concept for a larger study. Of the 174 patients initially screened only 50 were eligible to take part in our study. This was due to our strict exclusion criteria, which eliminated all patients with CV problems; this in itself illustrates the increased prevalence of CV conditions in RA patients. More patients in the placebo group were on methotrexate, but this was balanced by more patients in rosuvastatin group being on sulfasalazine. The differential influence of methotrexate and sulfasalazine on the surrogate markers we measured is not known.
The hydrophilic property of rosuvastatin compared with atorvastatin is well known, which makes it a potent treatment for cholesterol-lowering effect. The pleiotropic effects of statins are well demonstrated in both hydrophilic and lipohilic statins9,10 among non-RA patients. However, it is important to demonstrate the pleiotropic effects in the RA population using a hydrophilic statin like rosuvastatin. Our study does demonstrate that the rosuvastatin's pleiotropic effects cannot be translated into clinical practice in patients with RA.
Accelerated atherogenesis is a major cause of morbidity and mortality in RA. Although initial mean lipid values lay within the reference range, rosuvastatin at the dose of 10 mg/day, substantially lowered the total cholesterol levels and adverse events were comparable to placebo despite various DMARD usage and anti-TNF therapy. This in itself is an important message considering the need for cholesterol-lowering agents in the RA population. However, the statin's clinically relevant anti-inflammatory effects apart from CRP-lowering effect still remains questionable.
Supplementary material
The supplementary material accompanying this article can be found online at: http://smj.rsmjournals.com.
Footnotes
Acknowledgements
The authors would like to thank the Harkness Bequest and the Chief Scientist Office, Scotland, for funding, Astra Zeneca for providing crestor and placebo tablets and Mrs Morag Wilson, Research Nurse.