
Abstract
Non-medicine-assisted tracheal intubation in prehospital trauma is associated with a dismal prognosis. We wished to study the outcome of medical patients who underwent non-medicine-assisted tracheal intubation. This retrospective study of patients attending our university hospital emergency department was conducted over seven years. The tracheal intubation database was analysed to identify medical patients not in cardiac arrest undergoing tracheal intubation without medicines. Intensive care unit, hospital, 12-month mortality and patients’ residence at 12 months were recorded. Eighty patients were identified who met inclusion criteria. The most common reason for intubation was definite airway compromise due to decreased conscious level (62.5%), then respiratory failure (26.3%) and finally potentially compromised airway due to a decreased conscious level (11.2%). Eighty-eight percent of patients with a definitely compromised airway were successfully intubated at first attempt compared with 66.7% of patients with a potentially compromised airway or respiratory failure (P = 0.03). Of 75 patients with complete data, 30 (40%) were survivors at 12 months, with all but two (6.7%) living at home. Non-medicine-assisted laryngoscopy leads to an increased first time tracheal intubation failure rate in patients with intact airway reflexes and, therefore, cannot be recommended as best practice.
Introduction
In our emergency department, an overwhelming majority of non-cardiac arrest patients requiring tracheal intubation receive medicines to facilitate this, usually in the form of a rapid sequence induction. In some cases a patient may be so physiologically compromised that the use of medicines is deemed unnecessary or potentially hazardous. An observational study of prehospital trauma patients who had tracheal intubation performed without medicine assistance found that almost all died, 1 and it is accepted orthodoxy from anaesthetic practice that the use of medicines to obtund the laryngeal reflexes and the profound sympathetic stimulation that occurs during tracheal intubation are beneficial therapeutic goals, although there is remarkably little data on this. We could find no published data looking at long-term survival in critically ill medical patients who have been intubated without medicine assistance, a practice that was known to occur by the authors in our hospital. For the purpose of our study we defined medical patients as any patient who was not in cardiac arrest or had a traumatic injury or a surgical diagnosis. As medical patients comprise a majority of those requiring emergency tracheal intubation in our hospital, this study aims to specifically describe tracheal intubation in this group of patients with regard to intubation success and long-term survival. Long-term survival in this unstudied group might be as dismal as it is in prehospital trauma patients, i.e. one could perform tracheal intubation without medicine in patients who were unsalvageable. We performed this pilot study to provide data for planning a future national study.
Methods
This was a retrospective observational study conducted between January 1999 and March 2006 in the emergency department of the Royal Infirmary of Edinburgh. Every patient undergoing tracheal intubation without medicines in the emergency department was eligible for entry. Tracheal intubation in our emergency department requires the intubating doctor to complete an audit form produced by the Scottish Trauma Audit Group at the time of intubation. 2 The data on the form include the specialty of intubating doctor, if any senior supervision was present, the number of attempts required for intubation, details of any medicines used and clinical reason for tracheal intubation (e.g. respiratory failure, potentially compromised airway and actually compromised airway). The data from this form are then entered into a database. For quality assurance purposes all tracheal intubations carried out in the emergency department are reviewed by an emergency medicine consultant and a consultant in anaesthesia and intensive care medicine. Initial analysis of the database identified those patients not having a rapid sequence induction. Searching the database after those who had a rapid sequence induction were excluded identified those patients who were intubated without medicine assistance. We retrieved and reviewed each of these audit forms. From the audit forms we gained information on age and sex of our study group, clinical indication for intubation and success of intubation. We then interrogated case-notes, hospital and the intensive care unit (ICU) databases (WardWatcher) in our region for information on diagnosis and outcome. The WardWatcher database is used to collect data from all Scottish ICUs, and is overseen by the Scottish Intensive Care Society Audit Group. WardWatcher is used to collect a variety of data pertaining to a patient's ICU admission, including diagnosis, length of stay and place of discharge. For patients admitted to ICU, we used the diagnosis entered on the WardWatcher database. For those who were not admitted to ICU, we used the diagnosis obtained from review of the emergency department notes, hospital case-notes and judgement of the authors. For hospital survivors we sought to identify immediate place of discharge (normal residence, rehabilitation unit or nursing home) and 12 month survival. Local ethics approval was sought and waived for this study. Statistical significance was at the P < 0.05 level and Fischer's exact test was used when appropriate.
Results
During the study period, 2234 patients underwent tracheal intubation in the emergency department. Of these, 97 (4.3%) patients were identified from the database as not having a medicine-assisted intubation. After notes review we excluded 17 patients (9 who had sustained trauma or had a clear surgical diagnosis, 6 patients who we could find no survival data on, 1 patient who had a medicine-assisted intubation and 1 patient who underwent tracheal intubation during cardiac arrest). This left 80 (3.6%) patients for detailed review.
The median age of our cohort was 69 years old with a preponderance of women (56.3%). A summary of our data are presented in Table 1. The median age for patients who had taken a drug overdose was 33 years, compared with 74 years in patients with other diagnoses. Of those where APACHE 2 data are available (38 of 80) the median was 20.5 with a range of 8–48. The most common reason for intubation was definite airway compromise due to a decreased conscious level in 50 (62.5%) patients, followed by respiratory failure in 21 (26.3%) patients and then potentially compromised airway due to a decreased conscious level in nine (11.25%) patients.
Overview of study group

IQR, interquartile range
Tracheal intubation was successfully achieved on the first attempt in 80% of cases. All patients were successfully intubated and no more than three attempts were required in any patient. When stratified by clinical indication, patients with a definitely compromised airway due to a decreased conscious level were successfully intubated on first attempt more often than in both the respiratory failure group and the group with a potentially compromised airway due to a decreased conscious level (88% versus 66.7%, respectively; P = 0.02). Anaesthetists and emergency physicians successfully intubated the trachea at the first attempt in 80% (P = 0.3) of cases; however, only five of 80 (6.25%) tracheal intubations without medicines were performed by anaesthetists.
Of the 80 patients in our study, 37 (46.3%) survived to hospital discharge. We were able to identify long-term survival and place of discharge data for 75 patients (Table 2), and further analysis of our data will be of this group.
Survival by diagnosis
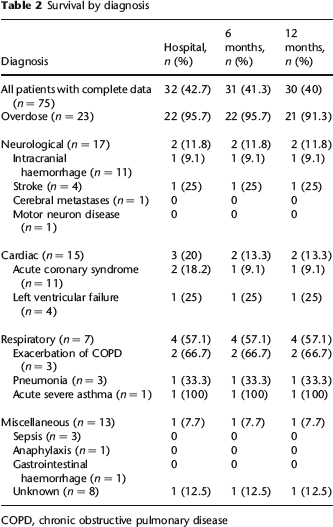
COPD, chronic obstructive pulmonary disease
Overall 32 of 75 (42.7%) patients across all diagnostic categories survived to hospital discharge with 30 of 32 (94%) surviving to one year. Only two patients were discharged to a long-term care facility, one with a diagnosis of drug overdose and one with a diagnosis of thromboembolic stroke; both were still alive at one year. In patients with a final diagnosis of drug overdose 22 of 23 (95.7%) survived to hospital discharge, with 21 (91.3%) surviving to one year. The next best survival was among those presenting with a respiratory illness; four of seven (57%) survived to hospital discharge and all were alive at one year. For patients with neurological or cardiac disease, hospital survival was far worse at 12% and 20%, respectively, but with only one further cardiac death by 12 months. No patient with sepsis, anaphylaxis or gastrointestinal haemorrhage survived to hospital discharge in our series.
Discussion
The practice of rapid sequence induction of anaesthesia for emergency tracheal intubation has been adopted as the technique of choice by a majority of anaesthetists and emergency physicians worldwide and is accepted as the gold standard due to its reliably high success rate.3–5 Our study has demonstrated that tracheal intubation without medicine assistance is performed infrequently in our institution, but when it does occur, it is overwhelmingly carried out by emergency physicians.
Fewer than one in two of the patients in our group of critically ill medical patients who underwent tracheal intubation without medicines survived to hospital discharge. However, a vast majority of those who survived to hospital discharge were discharged to their own homes and were alive at one year following hospital discharge. Therefore, the ability to perform tracheal intubation successfully without medicines did not correlate with the dismal outcome in the prehospital trauma patients. We believe we are the first group to report long-term survival data in such patients.
Tracheal intubation at first laryngoscopy was reported to be achieved in 82–86.9% of attempts using a rapid sequence induction technique in the emergency department.4–7 While these figures are only slightly better than ours (80% success at first attempt) when stratified by clinical reason for intubation, and patients with a definitely compromised airway are removed, first time success falls to 66.7% among those patients intubated because of a decreased conscious level causing potential airway compromise or respiratory failure. We hypothesize that those patients who do not have a definitely compromised airway are more likely to have intact airway reflexes, and thus it is more difficult to intubate their tracheas without medicine assistance.
An analysis of the National Emergency Airway Registry database (NEAR II) supports this view and found that a majority of failed intubations occurred when rapid sequence induction was not used as first-line airway management. 8 The administration of a neuromuscular blocking agent in addition to sedation has been shown to be associated with better intubating conditions,9,10 fewer attempts at laryngoscopy and fewer complications. 11 Multiple attempts at laryngoscopy in critically ill patients have been shown to be associated with hypoxaemia, regurgitation of gastric contents, bradycardia and cardiac arrest. 12 There is also some evidence that intubation without medicine assistance in patients with nontraumatic intracranial haemorrhage may be associated with a worse neurological outcome. 13 These have to be balanced against the risks of administering sedative and neuromuscular blocking medicines to a critically ill patient which include precipitating cardiovascular collapse and the development of a ‘can't intubate, can't ventilate’ scenario.14,15 However, we believe that the small risk of this scenario is vastly outweighed by the significantly greater risk of failing to intubate the trachea. Therefore, intubation without medicine cannot be considered best practice, especially in those patients who have potential airway compromise or respiratory failure.
Our study has several limitations. Single-centre studies have many inherent biases and our study is prey to all of these. Although the intubation audit forms are filled in at the time of intubation, we collected our data retrospectively and cannot validate the accuracy of the information. There were five patients for whom we could not obtain long-term survival data on. While it would have been ideal to formally assess quality of life using available validated tools, 16 due to the relative infrequency of a tracheal intubation without medicine assistance in our institution we collected data over a long time period, making this impossible in retrospect. We instead used place of discharge to home as a surrogate marker of a degree of independence. Furthermore, we cannot make any comment regarding the high mortality and the lack of use of intubating medicines as our study design is not appropriate to assess causation.
While our study cannot determine whether medicine-assisted tracheal intubation would have been beneficial in these patients in terms of survival, it is clear that tracheal intubation without medicine assistance in patients with intact airway reflexes is associated with more difficulty with tracheal intubation. In view of the morbidity associated with multiple attempts at laryngoscopy in the critically ill, we would not advocate attempts at tracheal intubation without medicine assistance even in patients presenting with a definitely compromised airway despite the reasonably high first time success rate in our series. We suggest that processes should be in place whereby necessary medicines, equipment and doctors with appropriate training in medicine-assisted tracheal intubation 17 are immediately available to manage critically ill patients requiring emergency tracheal intubation.