
Abstract
Menorrhagia is a common and important problem that has a significant impact on women's health. Menorrhagia is treated by surgical methods if primary medical methods fail. Surgical methods have changed over time and the traditional method of hysterectomy has been replaced by minimally invasive techniques. An examination of practice in Scotland suggests that minimally invasive techniques are now the most common surgical method of treating menorrhagia. Abdominal hysterectomies are still performed commonly, but the trend is towards a reduction in procedures performed annually. The changing technique of managing menorrhagia has an impact on the training of future gynaecologists.
Keywords
Introduction
Heavy menstrual bleeding or menorrhagia is defined as excessive bleeding from the uterus at the expected time of menstruation. Menorrhagia is a condition that has been shown to have a potentially important impact on the physical, emotional and social wellbeing of women. 1 Menorrhagia is a common problem. It has been estimated that one in 20 women in the UK between the ages of 30 and 49 years consults her general practitioner (GP) each year with menorrhagia. 2 Onward referrals of patients with menorrhagia from GPs to gynaecologists account for 20% of all referrals. 3
The management of menorrhagia comprises medical and surgical options. First-line therapies comprise hormonal treatments, antifibrinolytic (tranexamic acid) and nonsteroidal anti-inflammatory drugs (mefenamic acid). The National Institute of Health and Clinical Excellence (NICE) review on heavy menstrual bleeding recommends the levonorgestrel-releasing intrauterine system (Mirena) as first-line therapy for menorrhagia (Mirena) where an intrauterine system is acceptable to women. Treatment should, however, be tailored according to patient preference, fertility desires, side-effects and medical contraindications. Failure of primary therapies encourages consideration of surgical options in the management of menorrhagia. 1
The mainstays of the surgical management of menorrhagia are endometrial ablation and hysterectomy. Endometrial ablations have evolved over time and at present there are a variety of methods and techniques employed to destroy the endometrium. Endometrial ablation is minimally invasive and is regarded as a safe and effective alternative to hysterectomy offering high satisfaction, rapid recovery and low complication rates. 4 The type of ablation that is used is dependent on the cause of menorrhagia, operator preference and operator skill level. Submucous fibroids and endometrial polyps >3 cm and repeat ablative procedures are generally regarded as being more effectively treated by first generation techniques (transcervical resection of endometrium/fibroid or rollerball ablation), whereas regular uterine cavities are suitable for second generation technologies (e.g. novasure, microwave endometrial ablation or thermal balloon ablation).
Hysterectomy for menorrhagia can be performed abdominally, vaginally or with laparoscopic assistance. Hysterectomy, while guaranteeing amenorrhoea, exposes the patient to increased complications and a delay in return to normal daily functions when compared with ablation therapy. 5
The surgical management of menorrhagia has changed significantly over the last 20 years. Traditionally, the most commonly performed surgical procedure was a hysterectomy performed either abdominally or vaginally. Coulter et al. 3 showed that 60% of patients referred to a gynaecologist in the mid-1980s had a hysterectomy as treatment for menorrhagia. Endometrial ablation was introduced into UK practice in 1989 and has proved to be an effective alternative to hysterectomy with increasing popularity.6,7 The licensing of the Mirena coil as a treatment for menorrhagia in 2001 has proved to be a highly successful treatment of menorrhagia and has been shown to reduce the numbers of hysterectomies performed. 8 Reid et al. 9 showed that in England hysterectomy rates for menorrhagia fell by about a third over a decade (1989–2000). He argued, however, that this fall was not due to the introduction of endometrial ablation as significantly fewer operations overall were being performed for menorrhagia. He argued that it was the improvement in primary care and the introduction of the Mirena coil that accounted for the drop in hysterectomy rates.
Our aim was to observe the trends in the number of surgical procedures performed for menorrhagia in Scotland between the years 2000 and 2008.
Methods
We examined National Health Service (NHS) hospital episode statistics compiled from data submitted by all the NHS trusts within Scotland for the years 2000–2008. Data were included from patients treated in NHS hospitals only and, therefore, patients treated in the private sector are not included.
A disease code for menorrhagia does not exist in the international classification of disease code (ICD) 10th revision, so the code N92 (menstrual) was used. The following operation codes were used: Q17.4 (hysteroscopic destruction of endometrium) combined with Y08.8 and Y 11.1, Q17.6 (microwave endometrial ablation), Q17.7 (thermal balloon ablation of uterus), Q 17.1 (transcervical resection of endometrium), Q07 (all) (abdominal excision of uterus), Q16 (other vaginal operations on uterus), Q08.2 (vaginal hysterectomy) and Q08 (laparoscopicassisted vaginal hysterectomy) was combined with Y50.8 and Y75.1 and diagnostic codes N92 (menstrual) and D25.9 (fibroid). We analysed the data for patients between the ages of 20 and 55. The age range was used to minimise the risk that the data be contaminated with operations for non-menstrual indications. Transcervical resection of endometrium was classified in a group as first generation ablative techniques, while other techniques such as thermal balloon ablation, novasure and microwave endometrial ablation were combined in a group as second generation technique. Laparoscopic vaginal hysterectomy and vaginal hysterectomy were combined under the group of vaginal hysterectomy.
Results
The total number of operations performed for menorrhagia has increased by 25% between the years 2000 (4004) and 2008 (4926). The number of total abdominal hysterectomies performed for menorrhagia has decreased by a third in the same timeframe (3024 to 2000). Although first generation ablative techniques have remained constant over the past decade, there has been a significant increase in the number of second generation techniques used. The increase in these procedures has been 18-fold, up from 124 procedures in 2000 to just under 2100 procedures in 2008. Vaginal hysterectomy is the least common operation performed for menorrhagia, and the trend over the past decade is a gradual reduction in the number of procedures performed from 347 in 2000 to 214 in 2008 (Figure 1).
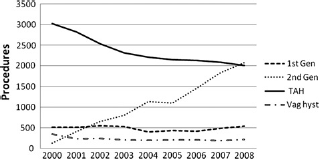
Surgical procedures for menorrhagia in Scotland, 2000–2008
Discussion
The total number of procedures performed for menorrhagia in NHS hospitals has increased significantly between the 2000 and 2008. This may reflect an increasing awareness among women of the availability of therapies to treat menorrhagia, but it has also been argued that the introduction of endometrial ablation has lowered the threshold for surgery. 10 Endometrial ablations are regarded as simpler to perform with a short learning curve and reduced complication rate particularly for second generation devices. Our figures would support this as it is the second generation techniques that have shown the most dramatic increase. The NICE has also encouraged the use of ablation as a primary therapy, particularly if menorrhagia has had a severe impact on the quality of life. 1 A further hypothesis is that the figures reflect a failure of the levonorgestrel intrauterine device as a first-line therapy. Kennedy et al. 11 has shown that over half of the patients who have a Mirena coil inserted in randomized studies go on to have a hysterectomy. The failure of the Mirena device to control menorrhagia would encourage an increase in endometrial ablation as a second-line treatment. The Mirena coil was licensed for treating menorrhagia in 2001, and our figures would suggest that since its introduction that it has not had an impact in reducing the number of surgical procedures being performed. Long-term epidemiological data on the impact of Mirena on hysterectomy rates is awaited.
The number of hysterectomies for menorrhagia has fallen significantly over the eight years that were examined. This is a likely result of a combination of factors. Improved confidence and training in ablative techniques has reduced the need for major surgery. It would also suggest that ablative techniques are effective as a longterm treatment for menorrhagia. NICE also recommends that hysterectomy be offered only when other treatment options have failed or are contraindicated.
The NICE suggests that the preferred route for hysterectomy be vaginal. This is associated with reduced complications, decreased length of stay in hospital and quicker postoperative recovery. 1 Our figures would suggest that this advice has not been adopted as the vaginal hysterectomy rates have remained steady over the last decade.
There are no data available to assess the impact that treatments in the private sector have had on the trends observed in the NHS. As an overwhelming majority of people in Scotland seek medical help from the NHS the impact of treatments undertaken in the private sector would not be expected to influence the observed trends significantly.
It should be recognized that there are limitations involved in the use of ICD coding for the examination of health episode statistics. Inaccuracies in coding may impact upon the results indicated. The Information Service Division of the NHS Scotland conducted an assessment of recording accuracy for menorrhagia (ICD 10 code N92) for the time period between 2004 and 2006 and found the records to have an accuracy rate of 88.2%. 12
Conclusion
Menorrhagia continues to be an important health-care concern for women. The approach to its management continues to be influenced by evolving techniques. Traditional approaches to its management are being replaced by minimally invasive techniques. This has an important influence on the training of future gynaecologists. Training for gynaecologists in the future will need to concentrate increasingly on minimal access techniques and less on the traditional methods of open hysterectomy. These techniques require more skill and, therefore, a longer learning curve is required to train gynaecologists to such a surgical standard.