
Abstract
Doctors’ knowledge provides the basis to support good practice in infection prevention and control. However, there exists a paucity of validated knowledge assessment tools that can be reliably employed to identify poor knowledge levels of Clostridium difficile infection (CDI) within populations of doctors, preventing the effective identification of knowledge deficiencies and focused targeting of educational interventions. Here, we describe a development process to validate a novel CDI knowledge assessment tool for doctors. Two previously published CDI knowledge questionnaires were amalgamated to produce a combined questionnaire. Content was further evaluated by a panel of CDI experts, producing the ‘Lothian’ questionnaire. These questionnaires were tested in control populations comprising either infection control nurse (ICN) specialists or non-clinically trained individuals, and a cohort of medical staff. We compared the efficacy of the ‘Lothian’ questionnaire against that of previous questionnaire reports. We found that all of the questionnaires studied significantly discriminated between non-clinical and clinical populations (ICNs and medical staff) (P < 0.001) and had similar levels of sensitivity and specificity in discrimination between these targeted populations. This study describes the development of a robust CDI knowledge assessment tool that can be used to evaluate knowledge levels among doctors, compare populations and assist the targeting of educational interventions and plot trends following such interventions.
Introduction
Clostridium difficile infection (CDI) is the most common infectious cause of health-care-associated diarrhoea. 1 The consequences of CDI are of great importance to both the individual and the health-care institution, as it entails a higher risk of additional infections, longer length of stay and potential ward closures in order to control outbreaks.2–5 Symptomatic CDI can increase patient mortality rates by 10 times or more 5 and surgical management, although required in only a minority of cases, has a grim prognosis with mortality rates ranging from 46% to 67%.6,7 Estimates suggest that CDI costs an average-sized district general hospital £400,000 and consumes more than 2000 lost bed days annually. 8 Recent studies have also demonstrated that the excess treatment cost for CDI patients over the four-year study period was £20,000,000 (€22,500,000). 9
A wide range of infection control measures have been introduced to address levels of CDI. While few have been assessed by randomized controlled trials, those with the strongest evidence base for CDI prevention include antimicrobial stewardship, glove use and hand hygiene (utilizing soap and water) (reviewed in Hsu et al. 1 ). Such diverse infection control interventions require a high level of health-care worker (HCW) knowledge to allow early recognition of risk factors and clinical features, appropriate investigations to be performed and subsequent management instituted in accordance with CDI guidelines and best practice.
The contemporary assessment of English National Health Service (NHS) CDI rates 10 suggests that, while reductions in incidence have occurred, the above measures are only partially effective. Effective infection control programmes have been shown to reduce infection trends, 11 but such measures may be more successful if supported by appropriate educational programmes targeting doctors who possess poor knowledge levels. 12
A robust CDI knowledge assessment tool could have many uses, including better identification and assessment of an individual's need for education, monitoring of the effectiveness of interventions and identifying trends and, finally, allowing comparisons of knowledge levels in different HCW populations, both locally and nationally. 13
Recent reports confirm a lack of knowledge of CDI among HCWs,14,15 but such studies may be undermined by the limited translational relevance they possess; the assessment tool employed within each study had been utilized in discrete HCW populations without repetition or having undergone a validation/development process. Furthermore, neither specify an appropriate level of knowledge or ‘pass’ grade. In addition, the authors of these studies have recently identified inaccuracies within the content of each other's assessment tools in the scientific literature. 16 All of these factors compound the difficulties of researchers and/or infection control specialists who may aim to use a published assessment tool to assess doctors’ knowledge of CDI for their own aims.
Given the previous controversies surrounding such assessment tools and in order to better assist in the provision of a robust assessment tool for use in the above aims, we developed a novel knowledge assessment tool for CDI knowledge among doctors through design of a validation process to confirm acceptability, accuracy and translational ability.
Methods
Previously published questionnaires by Aroori et al. 14 and Tsagkaraki et al. 15 were used to produce our assessment tools. All content was initially included; however, evaluation of the combined questionnaire identified statements that were duplicated or highly similar in both original questionnaires. For the purposes of design, these statements were amalgamated into one statement in order to produce the combined assessment tool. Additionally, statements were reformatted from their original standing order in source questionnaires and grouped into overall subject area sections in the combined questionnaire.
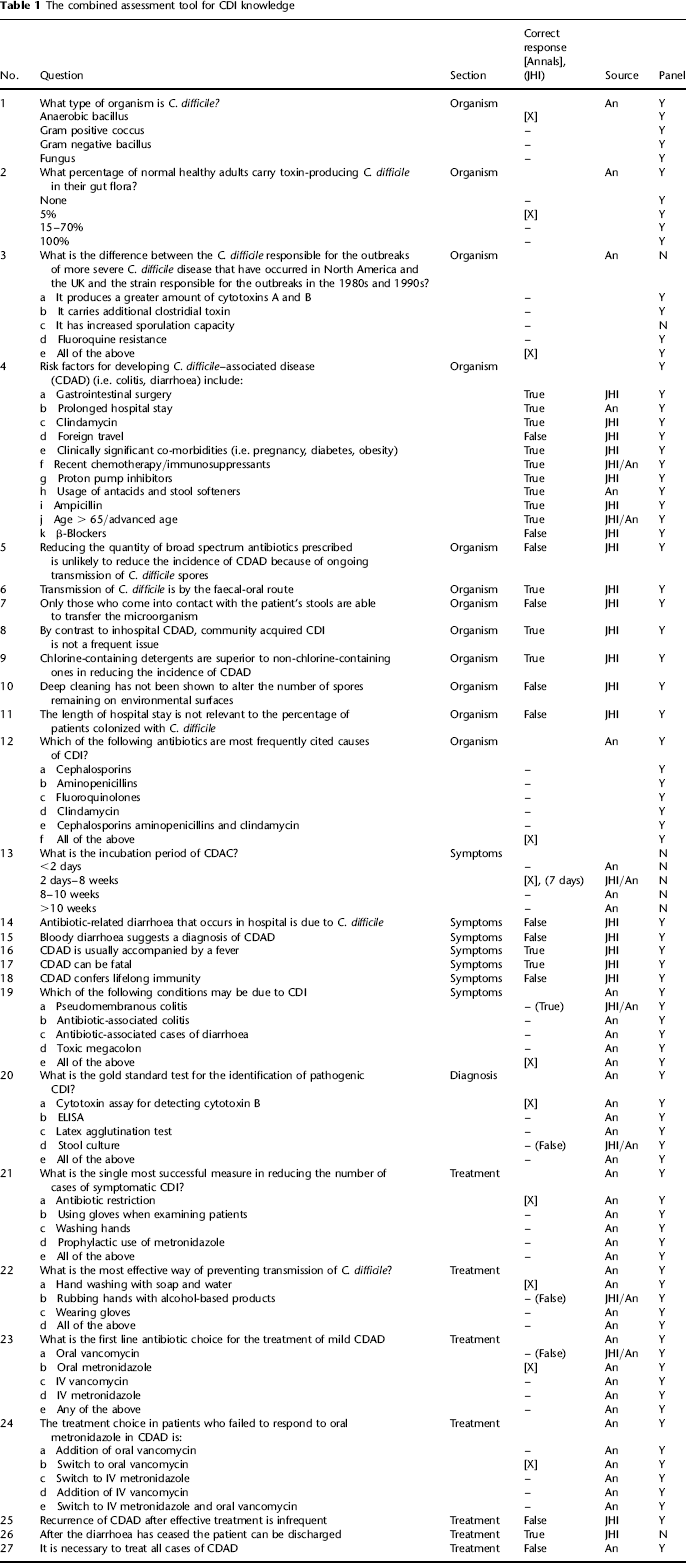
Content was then evaluated by a panel of five CDI experts (see Acknowledgements). Panel members were blinded to the origin of individual content statements and answers. They evaluated both the accuracy of each questionnaire statement and whether the statements represented an evaluation of reasonable expectations of basic CDI knowledge in doctors. Following this process, statements that were not felt to agree with the above provisions by a majority of panel experts were removed from the combined questionnaire to form a ‘Lothian’ questionnaire assessment tool (Table 1).
The combined assessment tool for CDI knowledge
To provide control populations with assumed low and high levels of CDI knowledge, respectively, and to compare previous questionnaires, the combined questionnaire was administered to a population of non-clinical scientific and administrative staff at the Medical Research Council Human Genetics Unit (MRC HGU), Edinburgh, and to a population of Infection Control Nurse (ICN) specialists. The non-clinical population was approached randomly at their place of work on the day of sampling, without prior notification, and asked to complete the questionnaire immediately online. ICN specialists working within NHS in Scotland were contacted directly by email through the Scottish branch network of the Infection Prevention Society (IPS). Subjects were asked to complete an online version of the combined questionnaire tool. All of the non-clinical subjects who were approached (n = 39) participated in the study; out of the 107 Scottish members of the IPS, 24 (22.4%) responded to the email request.
The questionnaire was trialed in a small cohort of Medicine of the Elderly doctors attending the April 2010 spring meeting of the British Geriatric Society (BGS) at the Edinburgh International Conference Centre, Edinburgh. Questionnaires were printed and included in the delegates’ welcome packs, and verbal announcements and reminders by the conference chair encouraged the attendees to complete the questionnaires individually and anonymously and return them to a marked collection point. Responses were received from 36 (7.8%) of the 461 delegates who attended.
For each respondent, we calculated the percentage of correct answers for each questionnaire. A missing response was considered an incorrect answer. In order to determine if there was a difference in the mean percentage of correct answers in the three groups, an analysis of variance (ANOVA) has been performed. As an ANOVA reveals whether there are differences between groups but not where those differences are, Tukey's test has been used to test pair-wise differences.
In order to identify whether there is an optimal cut-off in the percentage of correct answers within a questionnaire for distinguishing between groups, a receiver operator characteristic (ROC) curve has been produced and is presented along with area under the curve (AUC) and 95% confidence intervals (CIs) for the AUC. Statistical significance was accepted at P = 0.05.
This study was approved by the Lothian Regional Ethics Committee. The permissions for the various arms of this study were obtained from the relevant organizations (see Acknowledgements).
Results
Population demographics
Control populations were made up of 39 non-clinical scientific and administrative staff, 24 ICNs and 36 doctors attending the BGS conference in April 2010. Of the delegates attending BGS, 5.6% (n = 2) did not list a grade. Of the 34 who did, 44% (n = 15) were specificity registrars (SpRs), 41% (n = 14) were consultants, 9% (n = 3) were associate specialists and the remaining 6% (n = 2) were general practitioners (GPs).
Evaluation of statements by an expert panel
The combined questionnaire comprised 37 individual statements. Nine statements were sourced from the Aroori questionnaire and 21 from the Tsagkaraki questionnaire. In addition, seven statements on the combined questionnaire were generated as an amalgamation of two similar statements from both source questionnaires.
Three statements were deemed inappropriate by a majority of the expert panel: statement 3c (describing sporulation capacity of C. difficile; panel members did not feel this was a basic CDI knowledge requirement for doctors), statement 26 (describing discharge of a patient after diarrhoea had ceased; panel felt that more information was required before this could be answered with certainty, with a presumed assumption in this case that CDI had been the main cause of admission) and statement 13 (regarding C. difficile incubation; panel did not think that the answer to this was as clear cut within the current scientific literature).
In agreement with published criticism, the panel had difficulties with an Aroori question (question 19), 16 but thought that the question was appropriate if the answer was changed to ‘all of the above’, rather than as formatted in the source questionnaire. Similarly, while the panel felt that question 20 regarding laboratory diagnostics was appropriate, they recognized previous concerns 16 that this may be dependent on local practices and may require modification depending on where the questionnaire was being used. The panel also advised that future questionnaires should have slight modifications, including questions 8 and 16, which a majority of the expert panel felt would be improved by alternate wording that would clarify the statements.
Questions 3, 13 and 26 were therefore removed from the combined questionnaire to form a ‘Lothian’ questionnaire. All other statements were maintained in their original format in order to allow a representative comparison of source questionnaires through analysis of population responses of the combined questionnaire.
Evaluation of content in control populations
The percentage of correct answers gained per population for individual statements in the combined questionnaire is illustrated in Figure 1. As demonstrated, the trend for a higher percentage of correct answers achieved by ICNs and doctors is maintained throughout most statements; however, there are a number of areas of interest. In four statements (statements 8, 16, 20 and 21) less than 50% of ICNs got the answer correct. In addition, despite an absence of clinical training, 80% of non-clinical staff were able to answer the following statements correctly (statements 4a, 4b, 4f, 4k, 7, 17 and 18). These questions may therefore be appropriate to include in a questionnaire but may be non-discriminatory between populations.
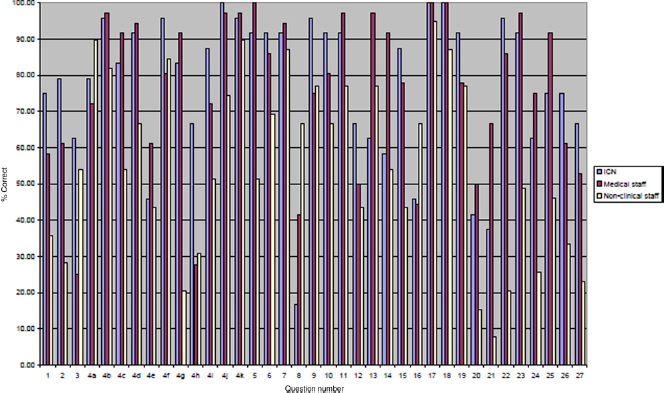
Percentage of correct answers per population for each statement within the combined questionnaire
While there was no overall statistical difference between the percentage of correct answers scored by doctors and ICNs, doctors tended to answer more questions correctly in the diagnostics and treatment sections than ICNs. The greatest difference between non-clinical and clinical/ICN population CDI knowledge levels was also to be found in the diagnostics and treatment sections (Figure 2).
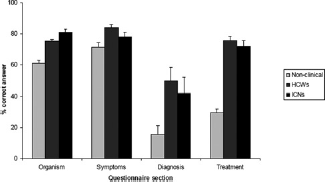
Comparison of population knowledge levels per questionnaire section (± standard error of the mean)
The mean percentage of correct answers achieved by doctors were 79.0% for consultants, 75.9% for registrars/trainees and 71.8% for others. Owing to the small size of this pilot population, these differences were not significant.
Comparison of questionnaires
The distribution of the percentage of correct responses from each population per questionnaire is illustrated in Figure 3. There is a significant difference in means across the groups (P < 0.001) for all questionnaires. In all questionnaires, assessments could statistically discriminate between non-clinical staff and doctors (P < 0.05) and non-clinical staff and ICNs (P < 0.05). No tested questionnaire could discriminate between ICN and doctor populations (P > 0.05).
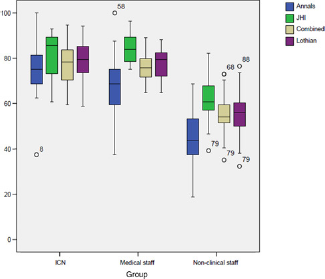
Boxplot of overall questionnaire percentage marks achieved per population
In order to establish whether there is an appropriate ‘pass mark’ to discriminate between non-clinical staff and ICN/doctor populations, an ROC curve was generated (Figure 4). There was no statistically significant difference between the Lothian and combined questionnaire AUCs (0.95; 95% CI, 0.91–0.99 and 0.96; 95% CI, 0.93–0.99, respectively) compared with the Aroori and Tsagkaraki questionnaires (0.93; 95% CI, 0.88–0.98 and 0.95; 95% CI, 0.91–0.99, respectively). A Lothian questionnaire pass mark of 63.2% (21 correct answers out of 34) allows the ability to distinguish between non-clinical staff and ICN/doctor populations with a sensitivity of 0.95 and specificity of 0.795.
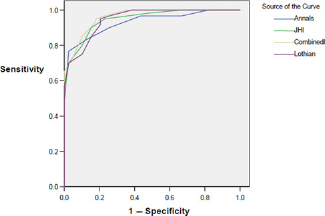
Receiver operator characteristic curve to determine cut-off point between non-clinical and ICN/doctors for each questionnaire
Discussion
This study aimed to develop and/or determine the most robust assessment tool to identify doctors who possess low levels of CDI knowledge.
To date, those who used a questionnaire to assess CDI knowledge had difficulty sourcing a validated assessment tool. This was due to the absence of any control populations, formal validation processes, repetition or acceptability testing of some of the previously published questionnaires. In addition, critics, including authors of such papers, have identified weaknesses in the content of previous questionnaire reports.
Here, we confirm that previously published questionnaires, irrespective of the above problems, will statistically discriminate between non-clinical and clinical/specialist populations. The process that we have undertaken has also provided a novel questionnaire assessment tool that has been evaluated by a panel of experts and undergone evaluation in control populations to confirm that the content is both accurate and acceptable in the evaluation of a population of doctors.
The statements were initially reviewed by an expert panel. Through this review process a number of statements were revealed to have factual difficulties, to have local practice variation or to require rewording to improve the clarity of the statements. These concerns were borne out in testing within the control populations when some statements generated answer patterns that were unexpected in the positive control population. The questions that caused these issues included questions 8 and 16, both of which the experts had recommended would require rewording, and questions 20, which was felt to be dependent on local practices. Future questionnaires may benefit from modifications to the statement content, with particular attention to local circumstances. The science and epidemiology of CDI are constantly changing; therefore, variation in policy or data by region or in future knowledge gain requires future questionnaires to be modified to reflect current and local knowledge. The difficulties of accounting for local circumstances or variations in practice have also been a feature of previous infection control knowledge questionnaire studies. 12
The small proportion of responses received from those at the geriatric conference was disappointing and is reflective of a response rate in voluntary questionnaire studies. While drawn from a wide national base of attendees, results could also reflect a bias within a geriatrician population towards those who attend conferences. In addition, there may well be a bias towards those who have greater knowledge of CDI and thus preferentially returned the questionnaire. This could explain why no questionnaire was able to discriminate statistically between ICNs and geriatricians. Therefore, no general conclusions in relation to knowledge levels of geriatricians as a population could be drawn without repeat testing in a larger population.
There was a small difference in methodology utilized between the different populations tested. Non-clinical and ICN populations completed an electronic form of the questionnaire, while the geriatricians completed a paper hard-copy. While all questionnaires were of identical content, we are unable to describe whether a different form of questionnaire could have any influence on a participant's score.
Future work, testing an updated questionnaire in a large cohort of hospital doctors of varying grades, would help further validate this CDI knowledge assessment tool.
Conclusions
Here, we describe the development of a robust CDI knowledge assessment tool containing previously peer-reviewed content, evaluated through testing in control populations and reviewed by a panel of experts. This questionnaire significantly discriminates between populations with assumed high and low levels of knowledge of CDI with quantification of sensitivity and specificity across a pass-mark range. This has relevance to those aiming to assess individual levels of CDI knowledge, compare levels within populations, identify risk factors for poor knowledge levels or evaluate trends over time and/or following interventions.
Footnotes
Acknowledgements
The authors thank the organizing committee of the BGS 2010 Edinburgh Spring Meeting, the staff and management of the MRC HGU, Edinburgh and Rona Broom and the Scottish Members of the Infection Prevention Society. In addition, the authors thank the panel of expert reviewers, which also included Dr Pota Kalima, Professor John Starr and Dr Karen McSween. This research was presented as a poster at the Federation of Infection Societies meeting in Edinburgh in November 2010.