
Abstract
Traditional methods of investigating suspected colorectal carcinoma (CRC) such as barium enema, colonoscopy and computerized tomography (CT) pneumocolon are often poorly tolerated by frail or elderly patients. Comparatively, minimal-preparation CT (MPCT) is a non-invasive investigation that does not require bowel preparation. The aim of this study was to review MPCTs carried out at the Western General Hospital, Edinburgh, and compare findings with current published data. Retrospective analysis of 85 patients (age range 55–99 years) who underwent MPCTs at the Western General Hospital between May 2005 and June 2008 was undertaken. Results were followed up using clinical notes, pathological and surgical databases. Subsequent outcomes were analysed (average follow-up 22 months). The prevalence of CRC within the study cohort was 0.14. Sensitivity of MPCT was 1 (95% confidence interval [CI], 0.69–1) with a specificity of 0.93 (95% CI, 0.84–0.97). Thirty percent of patients were found to have extracolonic findings requiring further investigation or intervention. Of the patients, 4.7% had an extracolonic malignancy diagnosed on MPCT. MPCT is a sensitive and specific method of investigating CRC in the elderly, infirm or immobile. Our results were found to be comparable with that of current published data, validating the service provided at the Western General Hospital.
Introduction
Colorectal carcinoma (CRC) is the third most common cancer in the world, after lung and breast cancer, with an estimated 1.23 million new cases diagnosed in 2008. It is the third most common cancer in men with 663,000 cases and 570,000 cases in women worldwide. 1 The number of new cases of colorectal cancer worldwide has been increasing rapidly since 1975. 2 In the UK, it is the second most common cause of cancer-related death and the third most common cancer, affecting more than 30,000 people each year with an average five-year survival rate of 40%. 3 It is a disease of advancing age with a greater than 10-fold increase in the incidence beyond 65 years of age compared with that under 65 years of age. 4
The investigation of the elderly, frail and immobile patient who presents with signs and symptoms suspicious for a colorectal malignancy is challenging as these patients frequently have difficulty tolerating formal ‘gold standard’ investigations such as barium enema and colonoscopy. The limitations also extend to the examination of the caecal region, which is the most difficult part to reach retrogradely and is prone to residual faecal contamination.5,6 While computerized tomography (CT) pneumocolon with virtual colonoscopy has been demonstrated to be more comfortable, and thus more acceptable, compared with colonoscopy and double-contrast barium enema, and it still requires bowel preparation, which is distressing to most patients regardless of the method of investigation. 7
In recent years, a number of papers have studied the use of minimal-preparation CT (MPCT) for the diagnosis of colorectal cancer in the elderly population.8–11 MPCT was first described by Day et al. in the early 1990s as an alternative technique for the imaging of the large bowel in frail elderly patients with suspected colorectal pathology who are referred for barium enema. The basic premise is that the detection of colonic cancer is important while the presence of polyps were of less clinical relevance. 8 Comparative studies have demonstrated MPCT to be reasonably sensitive (75–96%) and specific (82–94%) in detecting colonic malignancy.8,9
In this paper, we evaluate our experience using MPCT to determine if the sensitivity and specificity are replicable and in line with current published data. Table 1 discusses the pros and cons of MPCT, CT pneumocolon, barium enema and colonoscopy.
Comparison of CT pneumocolon with virtual colonoscopy, MPCT, double-contrast barium enema and colonoscopy

Methods
Dedicated MPCT reports of all patients between May 2005 and June 2008 were reviewed retrospectively. The results were obtained using APEX i. Lab services (Computer Sciences Corporation, Banbury, UK) and case-notes in order to determine pathological correlation, if any, and subsequent follow-up for any findings for an average period of 22 months (range, 14–24 months). The patient protocol for MPCT used in our institution utilizes 18 mL of meglumine and sodium amidotrizote (Gastrografin; Bayer PLC, Newbury, UK) diluted in 1.5 L water and taken in three divided doses in the 48 hours prior to the CT. A further 20 mL of gastrograffin in 900 mL was administered prior to the CT scan. No bowelcleaning agents or air insufflation was used. Intravenous contrast was also administered via pump injection. Helical CT acquisition of the abdomen and pelvis was then obtained using SOMATOM Sensation 16 (Siemens, Erlangen, Germany) from the domes of the diaphragm to the symphysis pubis utilizing 1.5 mm slice collimation, with 8 mm width and 2 mm reconstruction.
The MPCT findings were categorized into definite colonic malignancy, possible malignancy or no malignancy. A confirmed diagnosis was given following correlation with biopsy-proven colonic malignancy or polyp containing high-grade dysplasia or if there was overwhelming clinical evidence (e.g. colorectal mass with evidence of metastatic disease). For those with normal MPCT, the findings were deemed to be true negatives if no corresponding positive pathology demonstrated in case-note and results review.
False-positives were evaluated in terms of findings and adequacy of bowel preparation in order to determine if this had any bearing on results. The MPCT were also evaluated in terms of extracolonic pathology and the outcomes were reviewed with regards to extracolonic pathology and subsequent follow-up. Results were calculated using a standard two-by-two table with sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) as measures of diagnostic accuracy.
Results
A total of 85 patients (59 women and 26 men) were included in the retrospective review. The age range was from 55 to 99 years of age with an average age of 82 and a median age of 84 years.
Overview
A total of 17 patients were considered to have features consistent with CRC or ‘possible’ CRC and, therefore, were considered positive. A further 68 had no colonic findings and, therefore, were considered negative.
At the end of follow-up, 12 of the 17 positives had features consistent with a definite colorectal carcinoma. The remaining five were identified as having ‘possible’ malignancy; however, at subsequent investigation, they were diagnosed as having no malignancy (i.e. false-positive). Of the 68 patients considered negative on the MPCT, on follow-up, none were found to have colorectal carcinoma. These findings are summarized in Table 2.
Tabulated findings of the MPCT study cohort
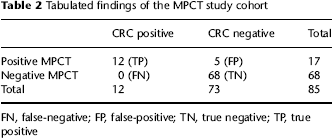
FN, false-negative; FP, false-positive; TN, true negative; TP, true positive
The disease prevalence in this cohort was calculated at 0.14. The sensitivity was calculated at 1 (95% confidence interval [CI], 0.69–1) and the specificity 0.93 (9% CI, 0.84
MPCT findings
Of the 12 positive cases, the majority was found in the caecum (43%), which is the most difficult to evaluate with colonoscopy or barium enema. The remainder of the distribution is summarized in Table 3. Of these, one of the 12 was found to have features of nodal spread. None of these 12 was found to have distant metastasis.
Positive MPCTs and outcomes
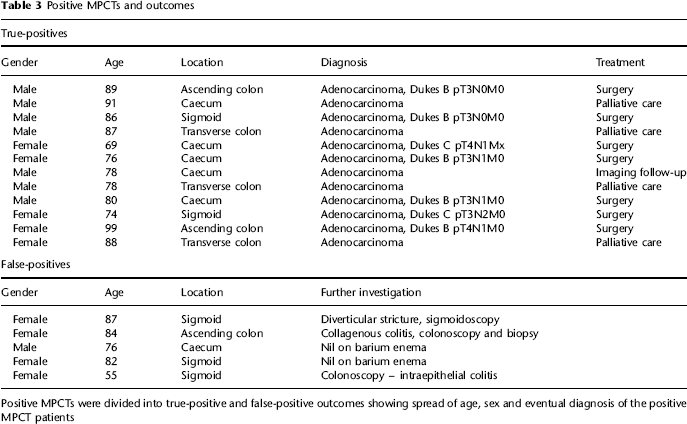
Positive MPCTs were divided into true-positive and false-positive outcomes showing spread of age, sex and eventual diagnosis of the positive MPCT patients
Of the 12 patients, seven underwent curative resection with four patients receiving palliative treatment. The remaining patient was considered too frail for treatment and underwent further imaging follow-up.
Of the false-positives, three were ruled out at colonoscopy/sigmoidoscopy and the remaining two underwent barium enemas. Two were found to have colitis (collagenous and intraepithelial colitis), one had findings due to diverticular disease and the remaining two had no mucosal abnormality and the uncertainty was likely due to poor opacification of the bowel with the oral contrast (Figures 1 and 2).
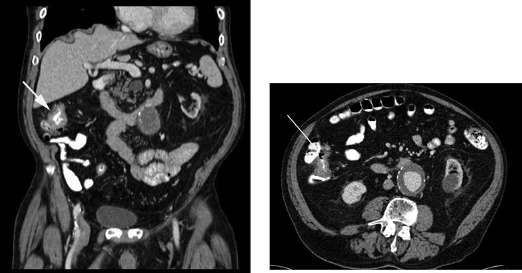
Coronal (left) and axial (right) MPCT demonstrating ascending colon thickening. The patient subsequently underwent a laparoscopic right hemicolectomy. This was Dukes’ B adenocarcinoma of the colon on the histology. Note the incidental 5.3-cm abdominal aortic aneurysm

Axial MPCT demonstrating transverse colon thickening. By biopsy this was proven to be an adenocarcinoma. The patient subsequently underwent palliative treatment
Extracolonic findings
A total of 26 of the 85 patients studied (30%) were found to have extracolonic pathology, which required further investigation or intervention were identified. This included a total of four extracolonic malignancies, which were pathologically confirmed on subsequent investigations (2 upper gastrointestinal, 1 ovarian and 1 lung adenocarcinoma). The findings are summarized in Table 4 (Figure 3).
Extracolonic findings within the study population

AAA, abdominal aortic aneurysm
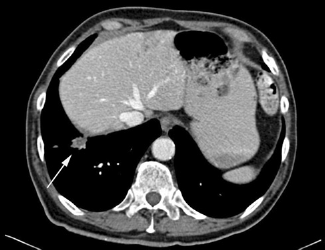
Incidental right lower lobe mass found on a MPCT study. This was subsequently biopsied and histology revealed a lung adenocarcinoma
Discussion
The investigation of the frail, elderly or infirm patient using the previously used ‘gold standard’ investigations of colonoscopy and barium enema is fraught with problems in terms of bowel preparation and patient tolerance. With regard to MPCT versus CT colonoscopy, MPCT does not require air insufflation or bowel preparation, which is better tolerated by the elderly patient. MPCT is a well-tolerated method with a high sensitivity and specificity with the added benefit of identifying extracolonic malignancies or pathology that may contribute to the patient symptoms. 12 While it is not sensitive enough to detect small colonic lesions or polyps less than 1–2 cm in size compared with CT pneumocolon or colonoscopy, although these may have malignant potential and may require removal in the younger patient cohort, polyps may take an estimated 5–8 years to progress to invasive carcinoma 13 and, therefore, is of less clinical relevance in the frail, elderly and infirm population. 8
While the study cohort at the Western General Hospital undergoing MPCT has been relatively small compared with studies based in Oxford and Cambridge, our results have yielded a favourable comparison with previously published data. The sensitivity and specificity have been well within the accepted range. The extracolonic malignancy detection rates have also been favourable with four extracolonic tumours detected, including one lung adenocarcinoma (Table 5).
Comparison of the results from the Western General Hospital with published studies on MPCT from 1993 to 2007
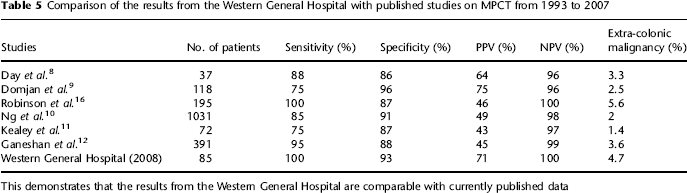
This demonstrates that the results from the Western General Hospital are comparable with currently published data
While the data with regard to the sensitivity have a wide 95% CI, this may be due to the difficulty in ‘establishing’ missed cancer in the study cohort as confirmatory tests were not generally sought in the aged population with CT-negative examinations. It is interesting to note, however, that while the patients were considered too frail for investigation by colonoscopy or CT colonography, one out of the 12, more than 50%, underwent resection for their colonic malignancy. This may be due to the advent of laparoscopic-assisted resection and enhanced recovery programme, improving perioperative survival.14,15
With the advent of the bowel screening programme in Lothian that began in May 2008 while MPCT has not incorporated as a second-line investigation following failed colonoscopy, it should be considered as a valid adjunct, especially for the infirm or frail patient within the age 50–74 years who are currently being offered participation in the bowel screening programme.
Conclusion
MPCT is a non-invasive and well-tolerated technique for investigation of CRC in the elderly or frail patient with the added benefit of detecting clinically relevant extracolonic pathology. The sensitivity and specificity of the MPCTs carried out at the Western General Hospital, Edinburgh, have been found to be comparable with the current published data.