
Abstract
Forearm fractures are common paediatric injuries. This study aimed to describe the epidemiology and treatment of paediatric forearm fractures in the urban population of Glasgow. We reviewed all forearm fractures treated by the orthopaedic service in Yorkhill Children's Hospital in 2008 up to the age of 13 years. Data were gathered from case-notes and radiographs using the prospective orthopaedic database to identify patients with forearm fractures. The age, sex, side and type of fracture, the timing and mechanism of the injury and treatment were documented for the 439 fractures. Census data were used to derive absolute age-specific incidences. Distinction was made between torus and other types of fractures. Torus fractures require no specific orthopaedic treatment and were segregated out. For the remaining 314 fractures, the age and sex distribution, seasonal variation of fractures and treatments for each type of fracture were examined. The incidence of forearm fractures in our population is 411 fractures per 100,000 population per year and 294 fractures per 100,000 population per year for non-torus fractures. An increased number of fractures occurred between May and August. A fall from less than 1 m was the most common mechanism of injury. Sporting injuries were the second most common. This study identifies some features which are in agreement with studies from elsewhere in Britain. However, there are also interesting differences, such as the Glasgow peak incidence for forearm fractures being at age eight, with a marked decline by 12 years. Furthermore, our findings have been extended to consideration of type of intervention and likelihood of successful treatment.
Introduction
Forearm fractures are common in children.1,2 We analysed all forearm fractures treated by the orthopaedic service in the Royal Hospital of Sick Children, Yorkhill, Glasgow, in 2008 up to the age of 13 years. The aim was to describe the epidemiology of paediatric forearm fractures in an urban population with respect to the mechanism of injury, seasonal variation, fracture classification and treatment.
Methods
Yorkhill children's hospital is in the city of Glasgow, which in 2008 had a population of 584,240. 3 The paediatric orthopaedic service manages patients up to the age of 13 years. The objective was to examine paediatric forearm fractures within the health district of Greater Glasgow. The population under the age of 13 years in 2008 was 106,772. 3 The published census data for age and sex allow calculation of age and gender specific incidence. 3 Yorkhill hospital receives additional patients from hospitals surrounding Glasgow – patients living outside Greater Glasgow were identified from their postcode and excluded from further analysis.
Information on all patients treated by the orthopaedic department is prospectively entered into a database by audit clerks. This database was used to identify all patients with forearm fractures in 2008, allowing review of all case-notes and radiographs for each patient. Patients were treated by one of five paediatric orthopaedic consultants. A single author (SWB) reviewed the radiographs and medical notes, and if the mechanism of injury was not documented, it was established by telephone contact. Torus fractures were identified as those failing in compression only, with no tensile failure on orthogonal views. For the apparently isolated radius and ulna fractures, the radiographic classification was confirmed by the senior author (JSH). The anatomical locations of fractures within the radius and ulna were classified into diaphyseal, metaphyseal and physeal fractures. Metaphyseal fractures were defined from antero-posterior radiographs as described by the Muller AO classification of fractures. 4 The proximal and distal metaphyseal segments of the bones were defined by a square, the sides of which have the same length as the widest part of the epiphysis; fractures occurring within this distance were classified as metaphyseal. Information collected included patient age, type and location of fracture, mechanism of injury and treatment.
The mechanisms of injury were divided into eight categories: blunt trauma, fall down stairs, fall of less than bed height (<1 m), fall of greater than bed height (>1 m), playground injuries, road traffic accidents, sport injuries and trampoline injuries. These categories are similar to those used in previous epidemiology studies.
Results
A total of 439 forearm fractures were treated by the orthopaedic service in 2008. In six patients with bilateral fractures, four were girls and two were boys. Fractures were more common in boys (249) than in girls (184).
Torus fractures are a common pattern of paediatric forearm fractures; they require basic immobilization as symptoms warrant and do not require orthopaedic management. In addition, the number of torus fractures is an under representation as a proportion would not be referred from the emergency department. Of the 439 forearm fractures, 125 (59 girls and 62 boys) were torus. In two girls and two boys, the torus fractures were bilateral. These patients were excluded from further analysis. In one female patient with bilateral fractures one fracture was a torus and this fracture was also excluded.
Of the 314 non-torus fractures, 89 (28%) involved the distal radius and ulna metaphysis, 178 (57%) the diaphysis and six (2%) the radial neck. Other fractures were comprised of 34 (11%) Salter Harris physeal fractures, three (1%) Galeazzi (2 girls, 1 boy) and four (1%) Monteggia (3 girls, 1 boy) fractures. Of these fractures, 188 (60%) occurred in boys and 125 (40%) in girls. There was one open fracture in the series (0.3%).
The incidence of each fracture type differed with age. The age distribution for all fractures (Figure 1), physeal (Figure 2), diaphyseal (Figure 3) and metaphyseal (Figure 4) are shown. The peak incidence for each of the fracture types differs.
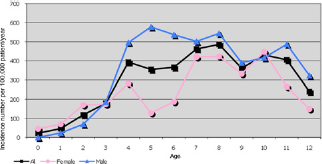
Overall incidence of forearm fractures

Incidence of physeal fractures

Incidence of diaphyseal fractures

Incidence of metaphyseal fractures
Fractures were more frequent in the spring and summer months between May and August (Figure 5), which is consistent with previous studies. 5

Seasonal variation of fractures
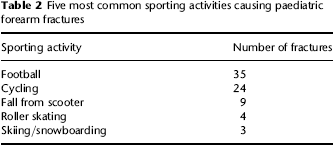
The most common mechanism of injury was a fall from a height of less than a metre (Table 1). There were 82 fractures associated with sporting activities with football being the most common (Table 2).
Mechanism of injury with number of fractures and type of treatment

MUA, manipulation under anaesthesia; RTA, road traffic accident
Five most common sporting activities causing paediatric forearm fractures
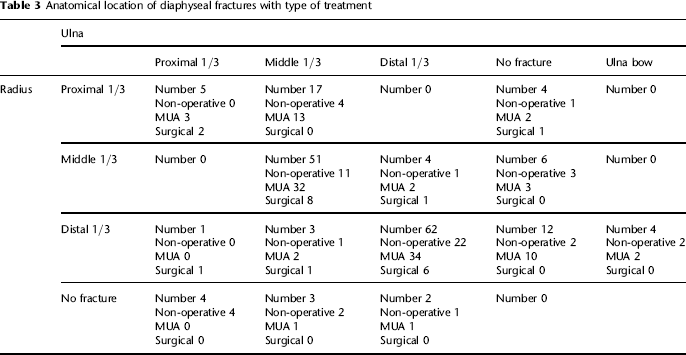
The 178 diaphyseal fractures were identified on radiographs and categorized into the injuries that affected either both bones or the radius or ulna individually. The anatomical location of these fractures was recorded and is presented in Table 3.
Anatomical location of diaphyseal fractures with type of treatment
There were 154 (49%) manipulations under anaesthetic for the treatment of forearm fractures (Table 4). Paediatric forearm fractures managed conservatively were immobilized in above-elbow casts (not routinely split). After manipulation under anaesthetic an above-elbow plaster-of-Paris cast was applied with the elbow in flexion and reinforced with resin prior to discharge. Five of these patients required re-manipulation under anaesthetic after they were judged to have displaced into an unsatisfactory position. Two further patients had K-wire fixation after manipulation. No physeal or metaphyseal fractures required re-manipulation. Out of the total of 161 patients treated with a manipulation under anaesthetic, 107 (66%) had diaphyseal fractures. Seven of these patients had a secondary treatment (re-manipulation, n = 5; secondary fixation, n = 2). This gives a failure rate of primary manipulation of 4.3% (7 cases of 161). All of the re-manipulations were required for diaphyseal fractures that were felt to have displaced to an unsatisfactory position, decided by the individual treating consultant.
Discussion
Studies have shown an increasing incidence of paediatric forearm fractures.2,6–9
A recent paper from Edinburgh by Rennie et al. 1 identified forearm fractures as 41.1% of all paediatric fractures. The incidence of forearm fractures in our population is 411 fractures per 100,000 population per year (439 fractures in 106,772 population). We identified the age-specific incidence for different forearm fracture types. This is a lower incidence that has been found in other studies. 1 This figure may be an underestimate as not all fractures in our hospital are referred to orthopaedics, with many torus fractures treated symptomatically in splints and discharged to primary care. The upper age limit of treatment in our hospital is 13 years, which is lower than that used in some other series. This means that our data do not include adolescent fractures, which we acknowledge makes direct comparison with other series difficult. Another factor contributing to our lower incidence is another hospital in the Glasgow area, the Glasgow Royal Infirmary, that may treat those paediatric fractures that do not warrant operative treatment.
Sixty percent of fractures occurred in boys. Fracture incidence peaked at eight years with a peak of five years for boys and 10 for girls. The different fracture patterns were found to have different age peaks. Diaphyseal fractures peaked at four years with a peak of five years for boys and eight years for girls. Metaphyseal fractures peaked at 10 years with a peak of 10 years for boys and seven years for girls. Physeal fractures peaked at 12 years with a peak of 12 years for boys and 10 years for girls.
There were similarities and differences to the fracture patterns identified in the epidemiological analysis of Rennie et al., although our data were limited to the 0–12 year age group. In the diaphyseal group, they described a bimodal distribution for boys and a unimodal peak for girls with the highest incidence between four and six years. 1 We identified a peak in diaphyseal fractures between the ages of four and six years for boys but could not identify a bimodal distribution in boys (as was described between 12 and 18 years). The peak age of female diaphyseal fractures occurred later in our study group at eight years. The distribution of metaphyseal fractures was similar with both female and male fracture incidences initially rising with age before tailing off. Female fractures reduced in incidence at an earlier age than in males.
The incidence of forearm fractures is low in the first two years for all fracture subtypes. If a forearm fracture is identified in this age group, the possibility of non-accidental injury must be considered and particular attention paid to the mechanism of injury. It should be noted, however, that no cases of non-accidental injury were identified in this study group.
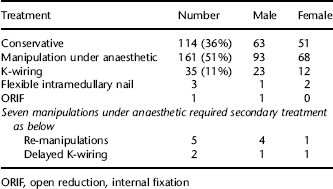
ORIF, open reduction, internal fixation
An increase in the number of forearm fractures was identified between May and August. This parallels the increase in paediatric fractures in the spring and summer months that has been previously identified. 5
Falls accounted for the majority of fractures. This is consistent with previous studies regarding upper limb fracture. 10 This study by Williamson et al. identified 47 out of 277 upper limb fractures secondary to road traffic accidents to only two fractures in our study. Both falls from over 1 m (n = 25 from 32 fractures) and trampoline (n = 20 from 23 fractures) injury groups had a higher proportion of children treated with manipulation under anaesthetic or surgical treatment compared with other mechanisms (n = 110 from 256 fractures). Twenty out of 23 forearm fractures sustained by children using trampolines required a general anaesthetic for treatment with 17 treated by manipulation, two by primary K-wire fixation and one by flexible elastic nailing. Of the 17 patients treated with manipulation, two patients required a secondary manipulation. This may reflect a higher energy mechanism of injury than occurs in other activities. The incidence of trampoline paediatric fractures has been increasing in the UK. 11
The five most common sporting activities associated with forearm fracture were football, cycling, fall from a scooter, roller-skating and skiing and snowboarding. These same five sports were identified as the most common causes of distal forearm fractures in 2000–2001 in the population under the age of 35 years. 2 A sport notable for its absence from the table is rugby, which is played widely in schools in the Glasgow area. One reason for this may be that our data are limited to under 13 years of age and rugby injuries may be more prevelant in the secondary school adolescent age range.
Diaphyseal fracture patterns were classified anatomically into thirds to identify the common fracture patterns. The most common patterns were middle 1/3 ulna and radial fractures (n = 51) and distal 1/3 radial and ulna fractures (n = 62). In 66% (n = 118 of 178) of diaphyseal fractures, the radial and ulna fractures occurred in the same 1/3 of the shaft. In the group of middle 1/3 radial and ulna fractures, 40 (of 51 fractures) required admission and treatment in the operating theatre. Therefore, when this fracture pattern is encountered by accident and emergency physicians, they should be aware of the high percentage requiring specialist treatment.
A finding in this study was 22 isolated radius and seven isolated ulna fractures distinct from Monteggia and Galeazzi fracture patterns. In the isolated radial diaphyseal fractures 12 occurred in the distal 1/3, six in the middle 1/3 and four in the proximal 1/3. In contrast, four of the eight isolated ulna fractures occurred in the proximal 1/3. A previous study from Harvard Medical School identified only 17 isolated radial fractures in a 32-year period and identified this as 27% of all diaphyseal forearm fractures. 12 In contrast, we identified a higher number of isolated fractures in our population in one year and this accounted for 16% of all diaphyseal fractures (n = 29 of 178). Three Galeazzi fractures were identified compared with the 21 isolated radial fractures. When assessing isolated radial fractures in paediatric orthopaedics it is crucial not to overlook an injury to distal or proximal radioulnar joints; however, isolated radial diaphyseal fractures can be treated without specific treatment to the distal radioulnar joint. A similar finding of a higher incidence of isolated radial shaft fractures over Galeazzi injuries has been identified in an adult series. 13 In our series, no isolated radial fractures treated by manipulation under anaesthetic required any secondary treatment. A previous study from Oxford by Gibbons et al. randomized 23 isolated distal radius fractures to manipulation under anaesthetic or manipulation and percutaneous wires. They found that 10 out of 11 isolated radius fractures treated with manipulation required re-manipulation, leading to the suggestion that these fractures should be treated with percutaneous wiring. 14 However, in this study isolated distal radius fracture was defined as a complete displaced diaphyseal fracture of the distal radius with an intact, buckle or greenstick fracture of the distal ulna making direct comparison to our cohort impossible.
It has been identified that the rate of percutaneous pinning has increased in the treatment of distal radius fractures. In Hong Kong, between 1985 and 1995, it increased from 9.5% to 38.7%. 15 A recent study by Flynn et al. identified an increase in operative treatment of diaphyseal forearm fractures from 1.4% to 10.6% between 1997 and 2008. In our study 18 out of 178 (10.1%) diaphyseal fractures were treated operatively, which is comparable with the findings in Philadelphia of Flynn et al. 16
A re-manipulation rate of 4.5% of diaphyseal fractures or 3% is consistent with previous studies showing 2.5% 17 and 4%. 18 A notable finding in this study was that none of the metaphyseal or physeal injuries treated by manipulation under anaesthetic required re-manipulation.
In our study, 64% of paediatric forearm fractures excluding torus fractures were treated in the operating theatre. In our hospital manipulation under conscious sedation in the accident and emergency department is not available and, therefore, manipulations require inpatient admission for treatment. Any increase in incidence will have an impact on requirements for inpatient resources in the future.
Paediatric forearm fractures are common and the incidence is increasing. This study identifies findings consistent with the epidemiological literature but has additionally shown previously unreported findings. We identified a peak incidence of forearm fractures at eight years, which is younger than described in other series. 1 We identified different ages for the peak incidence of different anatomical fracture types with diaphyseal at four years, metaphyseal at 10 years and physeal at 12 years. Forty of the 51 diaphyseal forearm fractures involving the middle 1/3 in both bones required surgical treatment associating this specific fracture pattern with the need for orthopaedic assessment. Football was identified as the most common sport associated with forearm fractures in the population of Glasgow.