
Abstract
Traumatic brain injury is a leading cause of death and disability in childhood. A retrospective study of all paediatric head injuries admitted to the neurosurgical unit for the West of Scotland over a 10-year period was performed to assess the impact of the National Institute for Health and Clinical Excellence head injury guidelines on the admission rate and to determine the associated risk factors, causes, severity and outcomes of these injuries. There were 564 admissions between 1998 and 2007. The median age at presentation was nine years and two months. There was no change in the admission rate, injury mechanism or severity of head injury admitted over the period studied. A relationship was observed between the Scottish Index of Multiple Deprivation Score and the incidence of head injury (P = 0.05). Alcohol was reported as a causative factor in only a small number of cases, and moderate to severe head injuries were more commonly identified as a result of road traffic accidents.
Keywords
Introduction
Traumatic brain injury is a leading cause of death and disability in childhood 1 and accounts for up to 500,000 paediatric admissions a year in the UK.2,3 Various factors have been reported to influence the incidence of these injuries, such as socioeconomic status, 4 gender 5 and age. 5 The paediatric head injury admission rate over a 10-year period spanning the publication of the 2003 National Institute for Health and Clinical Excellence (NICE) head injury guidelines 6 was studied to assess how these recommendations have altered our practice and determine the risk factors, cause, severity and outcomes of childhood traumatic brain injury admitted to the regional neurosurgical unit for the West of Scotland.
Methods
A retrospective study of head injury admissions from 1998 to 2007 was conducted using data collated from the departmental paediatric admissions database for children aged between six months and 16 years. The patients were divided by age into four groups: (1) between six months and less than one year old; (2) between one and less than five years old; (3) between five and less than 10 years old; and (4) between 10 and 16 years old. The mechanism of injury and the involvement of alcohol, the postresuscitation Glasgow Coma Score (GCS) and need for operative intervention were obtained directly from the database. The Glasgow Outcome Score (GOS) was derived from the first neurosurgical outpatient clinic letter. Patients whose injuries did not warrant review were assigned a GOS of five. All neurosurgical paediatric admissions were followed up by the paediatric outreach specialist nurse by either telephone or home visit.
Results
There were 564 admissions from 1998 to 2007. The median age at presentation was nine years and two months (range, 2 weeks–15 years 11 months) and 63% were men. The majority of the admissions were from hospitals within the Greater Glasgow and Clyde health boards with smaller numbers admitted from Ayrshire, Dumfriesshire, the Highlands and Islands and Forth Valley.
Admission rate
Figure 1 shows the total number of admissions for each year studied and demonstrates that there was no significant change in the annual number of admissions over the 10 years reviewed (P = 0.57). Although there appeared to be a decline in admissions in age group 2, as shown in Figure 2, the negative correlation was not significant. Similarly, the positive correlation in group 4 (10–16 years) was also not significant (P = 0.801). However, there was a statistically significant decline in admissions in age groups 1 and 3 (P = 0.0004 and P = 0.0021, respectively).
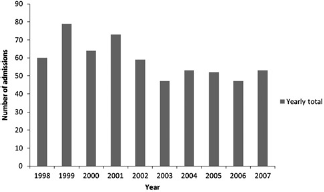
Number of admissions over the 10 years studied
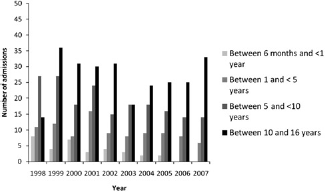
Number of admissions broken down into different age groups
Mechanism of injury and alcohol involvement
Table 1 shows the mechanism of injury and involvement of alcohol over the time studied. Data were incomplete for 28 patients. Falls account for over 50% of admissions, followed by road traffic accidents (RTAs) and assaults. Alcohol was involved in seven of the assaults, four of the falls and one of the RTAs (drunk driver). The youngest patient under the influence of alcohol at the time of injury was a 9.5-year-old boy who suffered a head injury secondary to an assault. All other cases involving alcohol were aged between 14 and 16. Cases involving alcohol were spread evenly through the time studied.
Mechanism of injury
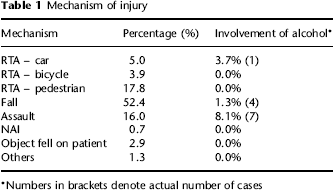
Numbers in brackets denote actual number of cases
Severity of head injury and outcome
The severity of the head injury was assessed by the postresuscitation GCS and divided into mild (GCS, 14–15), moderate (GCS, 9–13) and severe (GCS, ≤8). In total there were 399 admissions with mild head injuries, 85 with moderate and 78 with severe brain injuries. Data were incomplete for two patients. There is a significant negative correlation in the number of severe head injuries over the 10 years studied (P = 0.0116). However, the sample size is too small in this group to conclude that this represents a statistically significant difference. The frequency of mild and moderate injuries did not change with time (Figure 3).
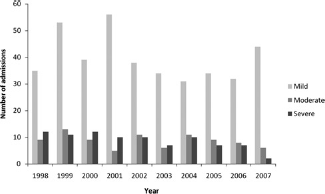
Severity of head injury admitted
The most serious injuries tended to result from RTAs (Table 2). Of the 78 severe head injuries, 48 were caused by RTAs (53%), compared with 33/85 (39%) of moderate head injuries and 81/399 (20%) in mild injuries. Of the 78 severe head injuries admitted, nine were due to RTAs involving the child as a passenger, six with a child riding a bicycle and 33 with a child pedestrian. It was not possible to ascertain the mechanism in 23 of 28 patients who died in the study.
Severity of head injury and mechanism of injury

It was not possible to ascertain the mechanism in 16 patients with severe GCS and two patients with moderate GCS
Interventions
Table 3 shows the interventions required to treat this population. Just under one-third of all admissions underwent an operative procedure (craniotomy, decompressive craniectomy, fracture elevation or suturing of lacerations). Twenty patients had intracranial pressure monitoring, several of whom then underwent further operative procedures.
Interventions
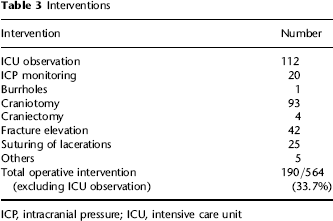
ICP, intracranial pressure; ICU, intensive care unit
Outcome
Outcome was assessed using the GOS. Table 4 shows the outcome for each severity of head injury. More severe head injuries were associated with poorer outcomes. The median length of follow-up was 3.5 months. Alcohol was involved in 1.52% of mild, 5.75% of moderate and 1.14% of severe head injuries.
Severity of head injury and outcome

Mortality
There were 28 deaths over 10 years. All suffered severe head injuries. The age range was 2–15 years, with a median age of 10 years. Mechanism of injury could only be ascertained in five of these patients. Two deaths were the result of gunshot injuries, two pedestrian RTAs and one fall.
Neuropsychology referrals
Of the 60 survivors with severe head injury, 28 (48%) required a referral for neuropsychology assessment compared with 18/85 (21%) survivors with moderate head injuries and 33/396 (8.3%) with mild head injuries.
Effect of NICE guidelines
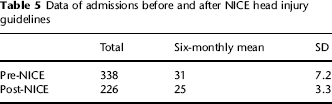
The NICE head injury guidelines were published in 2003. The numbers of admissions for the five years prior to and after this date were compared in order to assess the impact that these recommendations had on our admission rate. Table 5 shows the number of admissions before and after 2003; there is no significant difference between the two time periods (P = 0.96).
Data of admissions before and after NICE head injury guidelines
Scottish Index of Multiple Deprivation Score and head injury
The Scottish Index of Multiple Deprivation 7 is a method of allocating a deprivation score using the patient's postcode ranging from one (most deprived) to 6505 (least deprived). To aid analysis, we placed each patient into one of five quintiles depending on their deprivation score. Group 1 accounted for the most deprived 20% and group 5 the least deprived 20%. Around 17% of patients were excluded because of incomplete postcodes. Figure 4 shows the annual mean incidence of admissions/100,000 in each quintile (i.e. 1301 out of 6505 datazones). The median population in each datazone is 769. There is a correlation with the incidence of admissions with head injury and deprivation (P = 0.05).
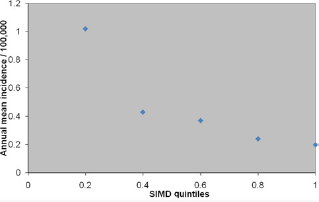
Admissions in each Scottish Index of Multiple Deprivation Score quintile. Lower quintiles denote greater relative deprivation
Discussion
Overall, paediatric head injuries admission rates have remained fairly stable over the last 10 years, with no significant changes in either the age of patient admitted or the severity of injuries seen. The NICE guidelines appear to have had no impact on our admission pattern. It may be that the Scottish Intercollegiate Guidelines Network (SIGN) head injury publication 8 in 2000 had already led to a change in the admission profile and so further change was not observed in this study. Interestingly, we are referred and admit a large number of mild head injuries and this practice has not changed with time. This is partly for geographical reasons as we have a low threshold for admitting head injuries from the Highlands and Islands because of the difficulties in imaging and transporting patients quickly from these remote areas.
As one might expect, the most common mechanisms of injury are falls, assaults and pedestrian RTAs, which is in keeping with the NICE findings. 6 The relative frequency of these mechanisms has not changed throughout the 10-year period, a finding that does not reflect the increasing media focus on teenage violence. In addition, as reported by NICE, pedestrian RTAs were more commonly associated with moderate or severe head injuries. As the admission rate of these injuries to the regional neurosurgical unit has not changed in frequency over the time studied, one must consider reassessing the initiatives implemented to reduce the risks of paediatric pedestrian RTAs. As well as child and parental education, Sharples et al. 9 suggested making safer play areas and restricting traffic in areas of high housing density. Grundy et al. 10 recently published data showing a significant reduction in the number of road casualties after the introduction of 20 miles per hour zones. Our data on head injuries in RTAs are in agreement with NICE data, despite the varied geography of the West of Scotland.
There is a clear correlation between head injury admission rate and socioeconomic status. Dunn et al. 11 already observed similar findings in the adult population in Scotland. In the deprived group (Group I) more frequent alcohol and substance misuse was noted and assault was more commonly reported as the cause of the head injury. The incidence of paediatric head injury has been reported to increase in larger families, 12 those families headed by a single parent 13 or in cases where mentally or physically ill parents care for the child. 14 The risk of death for child pedestrians has been reported to be four times greater in children from the lowest socioeconomic group. 15 It may be that, in the paediatric population, poorer parental supervision, inadequate parental education, gang culture and an increased frequency of alcohol intake both by parents and children all play a role in increasing the incidence of injury. Further studies would need to be performed to determine the relative contribution of these factors. However, in the present study the number of injuries occurring as a result of alcohol consumption is relatively small and does not seem to be rising. The majority of these cases are assaults or falls involving 14- to 16-year-olds. It seems likely that the alcohol consumption reported in this paper is an underrepresentation, as the potential consequences may deter children from admitting such behaviour.
A weakness of this study is the assessment of outcome in this population using the GOS. The relative frequency of neuropsychiatric referral hints at significant social and psychological problems even among those patients with mild head injuries. Previous papers have noted long-term cognitive and behavioural difficulties 16 in children with head injuries. Moderate disability following injury affecting a child's daily functioning has been seen in 43% of mild head injuries and 64% of moderate injuries. 17 Although the relation of the GOS and severity of head injury has been well described, it tends to underestimate morbidity in the paediatric population due to its emphasis on occupational/social activities and activities of daily living.18,19 Calvert et al. 20 suggest that the King's Outcome Scale in Childhood Head Injury 21 is a useful tool to estimate physical and cognitive needs at discharge. We will consider employing this scale prospectively in future studies.
Indeed, it may be that, as in adults with mild head injuries, children with acquired traumatic brain injury are more likely to have further medical and social problems. McMillan et al. 22 reported on the higher rate of death after head injury up to seven years after injury. The investigators felt that intervention aimed at changing lifestyle may help to reduce the continuing excess mortality. Further longitudinal studies are required to assess whether this observation of prolonged excess mortality is also seen within the paediatric head injury population.
The magnitude of the problem may be underestimated by this study as only a fraction of the head injuries are admitted to a neurosurgical centre. Further investigations with more detailed outcome scores as well as comparison studies with other centres within the UK will lead to a better understanding of the specific challenges we face when managing paediatric head injuries in the West of Scotland.