
Abstract
We present a case of Legionella pneumophila serogroup 3 (LP3) infection in a patient with severe community-acquired pneumonia (CAP). The diagnosis was complicated by an initial equivocal L. pneumophila urinary antigen test, followed by two negative samples. LP3 was cultured from a sputum sample and the diagnosis was confirmed by serology 15 days into the admission. This case highlights the importance of considering non-LP1 serogroups as causes of CAP and the role of serological testing in diagnosis.
Introduction
Legionellae are Gram-negative bacteria found in freshwater environments. Currently, there are over 50 species comprising 70 distinct serogroups in the genus Legionella. 1 Although half of all known Legionella species have been associated with human infection, Legionella pneumophila is responsible for approximately 90% of cases. 1 Currently, there are 16 serogroups of L. pneumophila. Marston et al. 2 found that 79% of all culture-confirmed or urine antigenconfirmed infections were caused by L. pneumophila serogroup 1 (LP1) with 3.6% associated with LP3. More recently, European surveillance data revealed similar results with LP1 responsible for 79.5% of legionellosis in 2007 and 2008. LP3 accounted for 3.2% of isolates obtained from culture-confirmed cases and was the second most common identifiable cause after LP1; 3 however, there is likely to be some geographical variation. For example, one study found that approximately 6% of clinical strains of L. pneumophila isolated in the Paris area belonged to serogroup 3. 4
Case report
A 62-year-old male patient presented with a one-week history of diarrhoea and vomiting and a 24-hour history of productive cough and shortness of breath. Significant medical history included obesity, ischaemic heart disease, hypercholesterolaemia and hypertension. Chest radiography at presentation revealed evidence of right upper lobe consolidation in keeping with pneumonia (Figure 1). He was pyrexial (38.4°C), tachycardic and tachypnoeic and had an elevated white cell count of 12.1 × 109/L (neutrophils 10.7 × 109/L) and a C-reactive protein of 406 mg/L. Creatinine was elevated at 154 μmol/L consistent with an acute kidney injury and serum sodium was 132 mmol/L. There was no history of foreign travel or infectious contacts. The working diagnosis was community-acquired pneumonia (CAP).
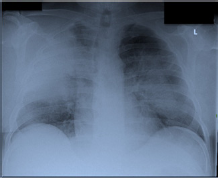
Admission chest X-ray revealing right upper lobar consolidation
He was admitted to hospital and commenced on empirical amoxicillin 500 mg eight hourly intravenously and clarithromycin 500 mg 12 hourly intravenously according to local protocol. On admission, routine sampling including blood cultures and sputum for bacterial culture were performed and a sputum sample was sent to the virology laboratory and a mid-stream specimen of urine was sent to the Scottish Haemophilus, Legionella, Meningococcus and Pneumococcus Reference Laboratory (SHLMPRL) for L. pneumophila urinary antigen testing. Samples sent to virology for polymerase chain reaction (PCR) and bacteriology for culture were negative. The Legionella urinary antigen enzyme immunoassay (EIA) (Binax; Inverness Medical, Bedford, UK) was reported as equivocal; however, the immunochromatographic assay (BinaxNOW; Inverness Medical) was negative. SHLMPRL requested a repeat urine sample for L. pneumophila antigen testing as well as a sputum sample for Legionella species PCR and culture in addition to serum samples for antibody testing.
Despite antibiotic and oxygen therapy, the patient deteriorated with increasing tachypnoea and deteriorating gas exchange. He was reviewed by the intensive care physicians and transferred to the intensive care unit for ongoing management. On day 3 of his admission, amoxicillin was changed to piperacillin and tazobactam 4.5 g eight hourly intravenously. Clarithromycin was continued until day 4, at which point it was empirically changed to moxifloxacin 400 mg 12 hourly intravenously. He underwent a trial of non-invasive positive pressure ventilation; however, he continued to deteriorate requiring intubation of his trachea and mechanical ventilation. Despite mechanical ventilation, his gas exchange remained significantly impaired. On day 4 of the admission the patient continued to be oliguric and a haemodialysis catheter was inserted into his left internal jugular vein to facilitate renal replacement therapy (RRT). Following institution of RRT, he was hypotensive and noradrenaline was commenced.
On day 4, SHLMPRL confirmed that the requested sputum sample was Legionella species PCR negative using primers that were not specific for LP1 but would be expected to detect DNA (16S rDNA) from any Legionella species. Two later urine samples were L. pneumophila urinary antigen negative by the Binax EIA. On day 7, his condition remained critical despite the aforementioned interventions; therefore, the antibiotics were changed empirically to meropenem 1 g 12 hourly intravenously (changed to 500 mg 12 hourly intravenously on day 8 due to acute kidney injury) and levofloxacin 500 mg 12 hourly intravenously. Subsequently, meticillin-resistant Staphylococcus aureus (MRSA) was cultured from the groin and linezolid 600 mg 12 hourly intravenously was added in order to treat possible MRSA pneumonia. By day 8 of his admission, oxygenation was critical and a referral was made to Glenfield Hospital in Leicester for consideration of extracorporeal membrane oxygenation (ECMO). He was duly accepted by the team at Glenfield Hospital and transferred on day 8. In Glenfield Hospital he received four days of therapy with ECMO during which time he continued to be ventilated with a ‘lung rest’ ventilation strategy. Following an eight-day admission to Glenfield Hospital he was transferred back to his base hospital for ongoing management.
On day 11 of admission, the base bacteriology department were notified that LP3 was cultured from the repeat sputum sample requested by SHLMPRL. The isolate was typed by the sequence-based typing method according to the protocols of the European Working Group for Legionella Infections (EWGLI) and found to be ST639 (6,10,2,28,9,4,6). There was only one other isolate with this ST type in the EWGLI database; this was a LP1 isolate from an environmental source in Sweden. Public Health were notified and an investigation was initiated to find a potential source of infection. After return to the base hospital from Glenfield Hospital, antibiotic therapy was rationalized to levofloxacin monotherapy, which he received for a total of 21 days. His transfer was uneventful and upon arrival at the base hospital he was breathing spontaneously with an FiO2 of 0.40 and an ongoing requirement for RRT. The patient continued to make steady progress and was discharged from hospital 40 days after admission. A serum specimen taken on day 3 of admission was negative by an immunofluorescence assay for Legionella antibody; however, a specimen collected on day 15 was positive at a titre of 2048 for LP3 and negative for LP1 (using an in-house test, antigens prepared by SHLMPRL), thereby confirming that the organism isolated was clinically significant.
Discussion
There are few documented cases of LP3 infection in the medical literature and no previous British case reports. A fatal case of LP3 was described by Watts et al. 5 in 1980 in an immunosuppressed patient with malignant lymphoma. In 2002, Oren et al. described a nosocomial outbreak of pneumonia caused by LP3 in four patients following haemopoietic stem cell transplantation in a two-week period. In all four cases, urinary Legionella antigen testing performed by enzyme immunoassay (Binax EIA) proved negative, and bronchoalveolar lavage (BAL) fluid cultured positive for LP3 8–12 days after the diagnostic procedure was carried out. 6 Between 1986 and 1987, 10 cases of nosocomial acquired LP3 pneumonia were idenitified in two hospitals in Paris, occuring primarily in immunocompromised patients. 7
Two separate cases of LP3 pneumonia in immunocompetent Japanese patients following near-drowning episodes in a hot spring spa have been described.8,9 In one of these cases, the initial Binax urinary Legionella antigen test was positive and a subsequent intratracheal specimen was culture positive for LP3. Only one of the cases had a significant rise in anti-LP3 antibody titres. LP3 was isolated from the spa water in both cases; therefore, this was thought to be the source of infection. Herpers et al. described a case of severe CAP in which initial urinary antigen testing for LP1 was negative and BAL specimens failed to culture an organism; however, L. pneumophila DNA was detected by PCR in the BAL washing. Repeat BAL did eventually culture LP3 in this case. 10
There are no studies that have specifically looked at risk factors for infection due to LP3, probably due to the fact that any study would not be adequately powered due to low prevalence. In the absence of specific risk factor data, it can be assumed that LP3 infection shares the same risk factors as infection due to LP1. Marston et al. 2 found that risk factors for legionellosis included immunosuppression, smoking, diabetes, malignancy, inreased age and end-stage renal disease. Other risk factors identified include male gender, surgery, recent travel (within 10 days of onset) and recent repair to domestic plumbing systems.2,11,12 The patient presented in this case report was a 62-year-old male obese smoker. It transpired that repairs were recently carried out on his shower after months of disuse; however, despite extensive water sampling, no household source of Legionella could be found.
Urinary antigen testing is the cornerstone of LP1 detection; however, PCR, culture and serology have an important role to play, especially in non-LP1 infection. British Thoracic Society (BTS) guidelines recommend that legionellosis be excluded in patients with severe CAP and recommends urinary antigen testing as well as culture of respiratory secretions. 11 BTS guidelines do recognize serology as a mechanism for identifying cases, however, although highly specific, there remains a high number of false-positives; therefore, it is not routinely recommended. Although PCR is described in the BTS guidelines, it is generally only available in reference laboratories and is therefore of limited practical use. 11 Despite this, molecular techniques such as PCR are gaining widespread popularity due to rapid turnaround times and diagnostic accuracy; however, this case illustrates the potential danger of relying purely on a negative PCR to rule out legionellosis. Although LP3 was finally cultured from sputum in this case, legionellae are fastidious organisms that are not readily cultivable from routine diagnostic media. In fact, Edelstein found that approximately one-third of clinical microbiology laboratories could not grow a pure culture of L. pneumophila. 13 This highlights the importance of high-quality respiratory samples in the pursuit of a culture-based diagnosis of legionellosis. Data from EWGLI revealed that serology was the main method of diagnosis in 20.9% of non-LP1 cases and 27.7% of non-L. pneumophila cases, compared with <10% for both culture and PCR. These data emphasize the continuing reliance upon serological diagnostic strategies. 3
The initial equivocal urinary antigen test is another intriguing aspect of this case. It has been reported that the Binax urinary antigen EIA can only detect LP1 antigen. 14 According to the manufacturer, the Biotest urine antigen EIA (Biotest AG, Dreieich, Germany) has a wide range of cross reactivity to L. pneumophila serogroups and other Legionella species. However, Benson et al. 15 reported that the Binax urinary antigen EIA had a sensitivity of 35% in detecting non-LP1, whereas the Biotest urinary antigen EIA had a sensitivity of 46%. Unfortunately, no isolates of LP3 were included in the study. Horn 16 performed a similar analysis including four LP3 isolates and found that the Biotest EIA detected 2/4 whereas the Binax EIA only detected 1/4. It is plausible that a urine specimen taken on admission, before antibiotic therapy had been established, would have an exceptionally high concentration of urinary antigen. This increased the likelihood that an antigen not identical to that for which the test was designed would be detected, albeit only equivocally. No matter which test is used, it is apparent that current urine antigen tests are not able to reliably detect non-LP1. This is of more importance in regions where the rate of non-LP1 infection is high or where outbreaks of non-LP1 infection occur. In our region, there has been a recent cluster of LP1 infections related to potting compost where serology played a substantial role in initial diagnosis and subsequent confirmation of the offending pathogen. 17
Conclusion
Remember that most L. pneumophila urinary antigen tests will only identify LP1;
Consider non-LP1 serogroups as potential aetiological agents in patients with severe CAP and negative or equivocal urinary L. pneumophila antigen tests;
Acute and convalenscent serology samples should be considered in all patients with severe CAP.