
Abstract
Acute myocarditis is an inflammatory disorder of the myocardium associated with cardiac dysfunction. The definition of myocarditis varies, but the Dallas criteria for myocarditis requires an inflammatory infiltrate and associated myocyte necrosis or damage not characteristic of an ischaemic event. Here we present a case of acute myocarditis in a 48-year-old woman masquerading as acute coronary syndrome. Patients with myocarditis usually have normal coronary arteries and we discuss diagnostic difficulties when it presents with ‘true’ acute coronary syndrome. In this case, cardiovascular magnetic resonance played an important role in the diagnosis of our patient and follow-up.
Keywords
Introduction
Myocarditis is an inflammatory disease of heart muscle. The leading cause of myocarditis is viral infection, but it may also result from autoimmune disorders, toxins and other infectious agents such as bacteria, spirochetes, fungi, parasites and rickettsiae. A definitive aetiology is rarely identified in clinical practice.
Case presentation
Following a one-day prodrome of sore throat, lethargy, diarrhoea and vomiting, a previously well 48-year-old white woman, presented with chest pain and collapse. Upon arrival of the paramedics her chest pain was ongoing and electrocardiogram showed left-bundle branch block, presumed to be new. She was therefore transferred to a coronary care unit for primary percutaneous intervention.
On arrival at hospital she exhibited features of cardiogenic shock. Coronary angiography revealed thrombotic occlusion of the distal left anterior descending artery. The coronary arteries were otherwise unremarkable with only minor plaque disease. Thrombus aspiration restored thrombolysis in myocardial infarction 3 (TIMI 3) flow (complete perfusion) in the distal left anterior descending (LAD) and no stent was deployed. Following the procedure, she remained in cardiogenic shock and required intensive haemodynamic support with intra-aortic balloon pump (IABP) and intravenous inotropes. Her admission troponin level was >50 μg/L (normal, <0.04 μg/L). Transthoracic echocardiogram was reported as showing moderate left ventricular systolic dysfunction (LVSD) with severe hypokinesis of the anterolateral wall. At this stage the working diagnosis was of acute anterior myocardial infarction with distal embolization of proximal plaque rupture. After recurrent episodes of pulmonary oedema and hypotension during attempts to wean her from IABP support, she was transferred to the Scottish National Advanced Heart Failure Service (SNAHFS).
A repeat transthoracic echocardiogram showed large wall motion abnormality extending from anterior septum to inferolateral wall. It was a particular concern that the patient's dire condition did not correlate with the angiogram findings and she subsequently had a cardiovascular magnetic resonance (CMR) imaging. It showed a non-dilated left venticle with moderate-to-severe systolic dysfunction and moderate mitral regurgitation, which was most likely functional in aetiology. On late gadolinium enhancement (LGE), there was widespread mid-wall hyperenhancement of the left ventricle with sparing of the inferior and inferoseptal walls (Figure 1). The distribution of the hyperenhancement corresponded to regional wall motion abnormality and the pattern was suggestive of acute myocarditis or established dilated cardiomyopathy. Following a period of aggressive diuresis with prolonged IABP support, her condition gradually improved and she was discharged.
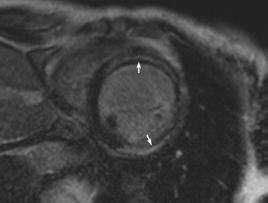
Gadolinium contrast-enhanced CMR scan; basal short-axis view demonstrating widespread mid-wall hyperenhancement (arrows) with sparing of the inferior and inferoseptal walls
She had a repeat cardiac MRI a month later which confirmed severe LVSD with ejection fraction of less than 25% and mild-left ventricular dilation; left ventricular end-diastolic volume measured 145.5 mL (normal, 52-141 mL). In contrast to the previous scan, the mid-wall hyperenhancement was less apparent with only a small sliver of non-hyperenhancing myocardium seen on the subendocardial side of the hyperenhancement. (Figure 2). The hyperenhancement which correlated with hypo and akinetic regions did not conform to any particular coronary artery territory and this appearance was consistent with remodelling following acute myocarditis.
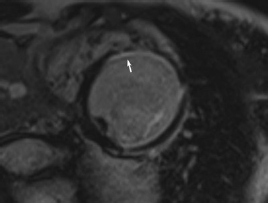
Gadolinium contrast-enhanced CMR scan demonstrating a less apparent mid-wall hyperenhancement with a small sliver of non-hyperenhancing subendocardial myocardium (arrow)
Discussion
The clinical presentation of myocarditis is highly variable 1 and this in part reflects the variability in histological disease severity. Myocardial inflammation may be focal or diffuse, involving any or all segments of the myocardium. Severe and diffuse myocarditis, as in this patient's condition, may result in acute dilated cardiomyopathy.
Signs of symptoms of myocarditis are largely non-specific and clinical manifestations include heart failure, chest pain, sudden cardiac death and arrhythmias. Cardiac enzyme elevation is present in 34-53% of cases2,3 and may often be mistaken for acute coronary syndrome, especially when presented with symptoms of chest pain and heart failure. Electrocardiogram and chest radiograph are often non-specific. The echocardiogram may detect reduced ventricular function in suspected myocarditis but is poorly sensitive and specific due to its suboptimal spatial resolution and provides minimal information on myocardial pathology.
CMR is a powerful non-invasive imaging modality which produces images with excellent spatial, soft tissue and temporal resolution. It can detect myocardial oedema and myocyte injury in myocarditis. Findings include increase in T2 signal intensity and LGE.4,5 The patterns of LGE in myocarditis can generally be distinguished from that in ischaemic cardiomyopathy: LGE in myocarditis preferentially involves the epicardium and mid-myocardium with sparing of the endocardium 6 and often in a non-coronary distribution. CMR can be used to guide myocardial biopsy and improve its sensitivity and, in certain cases, may obliviate the need for biopsy completely.
In our patient, the first CMR scan demonstrated moderate–severe left ventricular systolic dysfunction and widespread mid-wall hyperenhancement of the left ventricle with sparing of the inferior and inferoseptal walls. This pattern appeared inconsistent with an ischaemic myocardial insult especially in the context of areas of hyperenhancement which correlated with extensive regional wall motion abnormality which was not confined to a single LAD artery territory. The angiographic findings of a small calibre distal vessel occlusion was also unlikely to account for the severity of her presentation. Instead, supported by the appearance consistent with re-modelling following acute myocarditis in the repeat CMR, it seemed more likely that Mrs MM presented with an episode of severe acute myocarditis and coronary artery embolization of a left ventricular thrombus.
Thromboembolic phenomenon is not an uncommon feature in myocarditis and ventricular thrombus can be detected in 15% of patients on transthoracic echocardiography. 7 Myocarditis can mimic myocardial infarction clinically and is often suspected when it presents with a normal coronary angiogram. This case highlights the importance of suspecting acute myocarditis whenever a patient, especially one from younger population, presents with otherwise unexplained cardiac abnormalities of new onset, such as heart failure, myocardial infarction, cardiac arrythmias or conduction disturbances, even in the context of an abnormal coronary angiogram, especially when the findings are inconclusive, non-specific or out of keeping with the clinical presentaion. A history of recent upper respiratory tract infection or gastroenteritis may also be elicited in a majority of cases of viral myocarditis. CMR offers a powerful non-invasive method for assessing myocardial inflammation, which can greatly assist in the diagnosis of myocarditis and, in some cases, eliminate the need for biopsy. Although endomyocardial histology remains the gold standard for establishing the diagnosis, this case illustrates that a presumptive diagnosis may be given if the scenario and imaging studies are compatible and suggestive of the condition.