
Abstract
Digital acrometastases as a primary presentation of hepatocellular carcinoma (HCC) is rare. A 66-year-old man with no history of malignancy presented to the plastic surgery department with two skin lesions, one on the bridge of his nose and one on distal phalanx of left little finger. A working diagnosis of cutaneous metastases was made. Immediately prior to admission for excision of these lesions he was admitted with right upper quadrant pain and a jaundiced discolouration of the skin. The lesions were excised as planned and histopathological examination revealed metastatic HCC. A subsequent magnetic resonance imaging showed a lobulated mass consistent with primary HCC.
Case report
A 66-year-old man with a history of alcohol excess and smoking presented to the plastic surgery department with two skin lesions. One was on the bridge of his nose and another was on the distal phalanx of the left little finger. These lesions were highly vascular, exophytic in nature and rapidly enlarging. Surgical resection of the lesions was carried out with local flap closure to the nose.
The specimen for histopathological assessment consisted of the amputated tip of the left little finger, including the nail plate and an ellipse of skin from the nose. The specimen from the finger appeared diffusely infiltrated by tumour with a green discolouration to the cut surface, and bone was not identified macroscopically. The exophytic tumour on the nose measured 15 mm in maximum dimension and also had a green discolouration to the cut surface.
Histological examination of both lesions revealed similar features, which consisted of epithelial tumours with a mainly lobular architecture, including papillary elements and areas of rosette and pseudo-glandular space formation. The tumours occupied the dermis and subcutis and had no obvious epidermal component (Figures 1 and 2). In the sections taken from the acral tumour, virtual replacement of the bone was noticed. Tumour cells showed abundant dense cytoplasm, vacuolar round to oval nuclei with variable pleomorphism and conspicuous, mostly basophilic nucleoli. Mitoses were conspicuous (more than 20 per 5 high power fields), as was apoptotic activity. Abundant bile pigment was present within tumour rosettes (Figure 3).
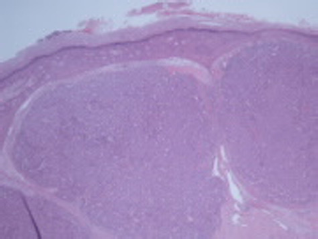
Low power view of the finger tumour demonstrating a lobular arrangement of tumour nests acini
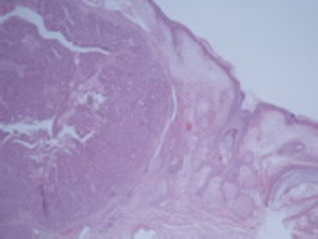
Low power view of the lesion on the nose showing a dermal tumour with solid and papillary areas
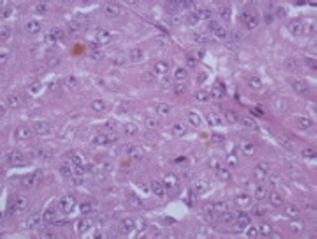
High power view of the finger tumour including mitotic pleomorphic and bile production
Immunohistochemistry showed that the lesional cells expressed the pan-cytokeratin marker MNF 116, and also the hepatocellular marker Hep Par1 (Figure 4). pCEA and CD10 were positive in a canalicular distribution (Figures 5 and 6). There was no expression of CK7, CK20, CK19 and CK14, TTF1 or melanocytic markers. The histological and immunohistochemical profiles were most consistent with metastatic hepatocellular carcinoma (HCC).
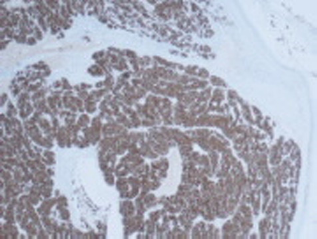
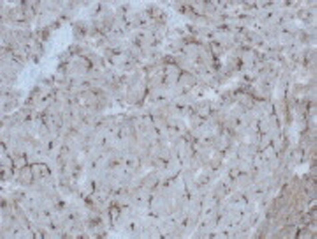
Strong and diffuse expression of Hep Par1 by tumour cells

Immunohistochemistry for CD10 demonstrating a canalicular pattern
Immunohistochemistry for carcinoembryonic antigen demonstrating a canalicular pattern
The patient was admitted with right upper quadrant pain and ultrasound abdomen was suspicious. Magnetic resonance imaging (MRI) of the liver was performed after surgical resection of lesions which was limited by the patient's inability to tolerate long periods lying in the scanner. However, the images obtained showed the presence of a lobulated mass measuring 7 × 3.5 cm in segment 4a of the liver. Further smaller areas of high signal were noted in segment 2 and segment 6. There was evidence of cirrhosis of the liver with nodular margins and moderate ascites. In view of his above-mentioned clinical risk factors, the MRI was finally reported as a multifocal HCC on a background of cirrhosis. His liver functions tests were deranged and results of viral, metabolic and immunological screens came back normal. Serum Alfa fetoprotein was 12 kU/L (normal range is ≤7 kU/L). Unfortunately the patient died within eight weeks of diagnosis due to communityacquired pneumonia and acute decompensation of chronic liver disease.
Discussion
The most common sites of extrahepatic metastatic HCC are the lungs, abdominal lymph nodes and bones. 1 The most frequent reported sites of bone metastases are to the ribs, spine, femur, pelvis and humerus, respectively. 2 Acrometastatic lesions of the fingertips are very unusual and even more so as the presenting manifestation of HCC. Following a review of the medical literature we have established that this is the first report of acrometastasis heralding HCC. A case of multiple cutaneous metastases over fingers, palms, toes, soles and back has been previously reported. Acrometastasis to the hands is uncommon, accounting for approximately 0.1% of all metastatic osseous involvement 3 and, according to some reports, the third finger is the digit most affected by osseous secondaries. 4 The most common cause of secondary osseous lesions is lung cancer followed by renal and breast cancer. It is also worthy of note that, because cancer patients are experiencing increased longevity, there is a greater opportunity for metastases to develop throughout the body. 5
Given the uncommon secondary involvement of acral sites, a diagnosis of acrometastasis is not necessarily clinically considered when investigating an unusual lesion on the hands. Cutaneous metastases from HCC are also very rare and in one series the overall cutaneous metastatic rate for HCC was estimated to be 0.8%. 6 Cutaneous metastases show protean morphological features with the face and scalp being the most common sites of involvement. In one study by Peters, 7 skin metastases were shown to account for only 2.7% of cirrhotic HCCs and no cases in non-cirrhotic HCC. Metastatic lesions may be the presenting sign of the HCC, but their occurrence is rare according to the medical literature, and to our knowledge there have been only 12 previously reported cases as a primary presenting feature of HCC. 8
The prognosis of metastatic HCC patients is generally very poor; however, there have been long survivors. Their prognosis correlates well to intrahepatic factors (i.e. primary cancer status and hepatic reserve). The median survival period is 4.9 months (range, 1-37 months). The mortality rate due to organ insufficiency as a consequence of extra-hepatic metastases from HCC is 11%. 9 According to the cases studied by Couto et al., 10 although most of their patients with unresectable HCC died as a direct result of cancer progression, 43% of patient died from complications of their cirrhosis, including sepsis, gastrointestinal bleeds and renal failure.
Acrometastases generally accompany widespread disease; hence they are associated with a poor prognosis. Survival has not always been reported in the previously published literature; however, based on cases that have been reported about outcome, the mean survival of the patients was six months. Our literature review shows that a diagnosis of hand metastasis is an indicator of poor prognosis. 11 Because of poor prognosis, palliation of symptoms is often the primary objective of treatment in these individuals. Amputation, external beam radiotherapy, chemotherapy and wide excision are the forms of treatment used most often.
Conclusion
This case report presents an unusual presentation of HCC. The occurrence of metastatic cancerous lesions within the hands carries severe prognostic implications. This case emphasizes the importance of awareness of uncommon manifestations of HCC.