
Abstract
Sacral nerve stimulation (SNS) has become an established treatment option for patients with intractable detrusor overactivity and non-obstructive urinary retention. The Scottish Sacral Nerve Stimulation service was established in April 2010 to provide a service for the population of Scotland. We report our experience from the first year of this new national service. All patients referred for SNS from the inception of the service in April 2010 until the end of March 2011 were studied. During the one-year period, there were 50 referrals. Thirty-three percutaneous nerve evaluations, eight tined lead tests and 16 permanent implantation procedures were performed during this period. Morbidity was low and both incontinence and quality-of-life questionnaires demonstrated statistically significant improvements (International Consultation on Incontinence Questionnaire [ICIQ-SF], P = 0.005; Incontinence Impact Questionnaire [IIQ 7], P = 0.0007; Urogenital Distress Inventory [UDI 6], P = 0.0002). Referral pattern was skewed towards the west of Scotland with some health boards producing no referrals during the year. Results from the first year of the service have shown that it is a safe and efficient procedure with significant improvement in incontinence, voluntary voiding and quality-of-life parameters. The limitation of funding for permanent implants inevitably impacts on the role of the technique as a management option in these patients.
Introduction
Sacral nerve stimulation (SNS) has now become an established treatment option in urology practice. It was first described in 1988 by Tanagho and Schmidt 1 and the technique was approved by the Food and Drug Administration (FDA) in the USA in the late 1990s and by the National Institute for Clinical Excellence (NICE) in the UK in 2004. 2 There are two groups of patients who may benefit from SNS: (1) patients who have intractable detrusor overactivity with symptoms of urinary frequency, urgency and urge incontinence and (2) patients who have non-obstructive urinary retention. Both conditions affect females predominantly.
Patients with intractable detrusor overactivity have typically undergone trials of conservative treatments including bladder retraining, anticholinergic medication to the maximal tolerated dose and intravesical botulinum toxin treatment. Many are at the stage of considering some form of urinary diversion or augmentation cystoplasty; major surgical procedures associated with morbidity and mortality. SNS is a totally reversible technique, which does not preclude further treatment, should the need arise. Several studies have demonstrated the safety and efficacy of SNS at short-term, medium-term and long-term follow-up. 3 5
The Scottish Neuromodulation Service started in April 2010, replacing the West of Scotland Service which had been in existence since 2008. The aim of the service is to provide a comprehensive sacral nerve stimulation service for urinary dysfunction for the population of Scotland. We report our experience from the first year of this new national service.
Methods
The Scottish SNS service is funded centrally by the National Services Division (NSD) and is based at the New Victoria Hospital, Glasgow. The patient care pathway is illustrated in Figure 1.

Patient pathway. GA, general anaesthetic; LA, local anaesthetic; OP, outpatient
Referrals from all regions of Scotland are reviewed at a multidisciplinary team meeting attended by two consultant urologists, our clinical physicist and our clinical nurse specialist. Based on the referral letter, a decision is made either to arrange a clinic appointment or to return the patient to the referring clinician as being inappropriate for SNS.
Most patients have a ‘one-stop’ appointment for initial consultation, urodynamic assessment and preoperative anaesthetic assessment. Following this, the patient may be booked for a percutaneous nerve evaluation (PNE), a tined lead test or returned to the referring clinician.
In a PNE, an insulated thin wire is placed under an anaesthetic into the third sacral nerve (S3) foramen on either the right or left side. This temporary unipolar lead is taped to the skin surface and connected to an external stimulator for a period of 2-4 weeks. If there is at least a 50% improvement in the main voiding or filling symptom, the temporary lead is removed and a permanent lead and pulse generator are implanted.
In a two-stage procedure, a tined (permanent) lead is implanted and tunnelled before connection to an external stimulator. The tined lead has four electrodes (Figure 2) and small tines or wings to keep the lead in place. This allows a more robust and reliable test. If the test is successful, the tined lead is then attached to the pulse generator which is implanted subcutaneously.

Tined test lead and lead insertion into the third sacral foramen (courtesy of InterStim Visuals)
Both PNE and tined lead tests are performed either as a day case or with an overnight stay. Patients are then reviewed either in person or by telephone. Implantation of a permanent SNS device is most commonly performed under general anaesthesia. Details of the techniques have been described previously by Spinelli and Sievert. 6
Programming
The pulse generator can be set at either a monopolar or bipolar setting. In monopolar stimulation, therapy current flows between one of the four electrodes and the pulse generator box itself. In a bipolar setting, two of the electrodes on the quadripolar lead act as anode and cathode. The ultimate aim of programming of the pulse generator is to arrive at a symptomatically satisfactory bipolar stimulation, which consumes less energy compared with a monopolar setting. To select the appropriate two electrodes, each of the quadripolar electrodes is tested in turn with a monopolar setting, using the pulse generator as anode. A series of bipolar settings can then be programmed until the optimal result is achieved. A minimum of three programming visits is required in the first year following implantation. Thereafter the patient is reviewed as required. Programming is thus a significant component of the overall process.
Assessment of success
Test implants are evaluated by comparing seven-day voiding diaries from the baseline (preimplant) and the stimulation periods. These diaries assess 24 hour frequency, volume voided, incontinence episodes and catheterizations (in the non-voiding cases). These diaries are scanned electronically by a bespoke system which was developed by one of the authors (DS). Successful tests are deemed to be those that show greater than 50% improvement in one of the above-mentioned parameters or removal of the requirement for catheterization.
All patients with permanent implants are followed up on a six-monthly basis by: Incontinence Impact Questionnaire (IIQ 7), Urogenital Distress Inventory (UDI 6) and International Consultation on Incontinence Questionnaire (ICIQ-SF). In addition, all implanted patients are asked to complete a three-day voiding diary on an annual basis.
Database
Management of the service is aided considerably by a database created specifically for this purpose. All the statistics for our annual reports are output as queries from this database, saving considerable time. In troubleshooting programming clinic situations, all details of past programming configurations are available. Urodynamics traces and X-rays can be viewed as images from hyperlinks. The ongoing quality-of-life assessment is also managed from the database. Automatic reminders are generated when quality-of-life assessments are due and, with only a minimum of manual input, the box and whisker plot shown in Figure 3 can be automatically generated.
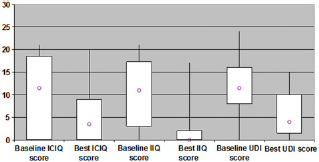
Comparison of baseline (pretreatment) and best quality-of-life scores (box and whiskers show median, quartiles and range)
Statistics
Descriptive statistics are illustrated by box and whisker plot, median and quartiles and significance testing by Wilcoxon signed rank sum test.
Results
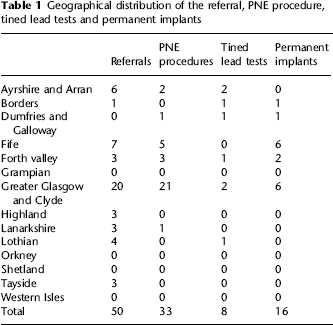
There were 50 new referrals from the areas covered by 10 Scottish Health Boards for the period April 2010 to end of March 2011 with a mean age of 48.2 years (range 21-79; Table 1). Five patients were returned to the referrer as being unsuitable for treatment based on the referral letter. Of 45 patients seen in the clinic, 38 patients (84%) proceeded to test stimulation. There were 33 PNE procedures, eight tined lead tests and 16 permanent implantation procedures (a further 3 patients who have had successful test stimulation proceeded to permanent implant after April 2011). During the year there were 119 outpatient follow-up visits.
Geographical distribution of the referral, PNE procedure, tined lead tests and permanent implants
Eight PNE patients proceeded to a permanent implant, giving a conversion rate of 45%, whereas all eight patients who had a tined lead test proceeded to a permanent implantation (100%). There was a statistically significant improvement in incontinence and quality-of-life parameters in patients who received permanent implants (ICIQ-SF median improved 7 points, P = 0.005; IIQ 7 median improved 11 points, P = 0.0007; UDI 6 median improved 7 points, P = 0.0002). All nine patients who were implanted for non-obstructive urinary retention are voiding satisfactorily at follow-up. Incontinence and quality-of-life questionnaire results are illustrated in Figure 3.
There have been two health-care acquired infections. In one patient (n = 1/16), the permanent implant became infected and despite prolonged antibiotics, was removed along with the tined lead. Another patient, having a tined lead test (n = 1/8), developed an infection of the lead with erosion of the lead through the skin. This was also removed.
Discussion
SNS is an effective and safe technique used to manage intractable detrusor overactivity and non-obstructive urinary retention. Overall, results are comparable with recently published studies.7,8 Van Kerrebroek et al. 3 reported outcomes in a large multicentre study of 152 patients. After a five-year period 68% of patients with urge incontinence, 56% with urgency frequency and 71% with urinary retention had successful outcomes, as defined by a greater than 50% improvement from baseline. Furthermore, no life-threatening or irreversible adverse events were reported. Using disease specific outcome assessment tools we have shown that there has been a statistically significant improvement in incontinence and quality of life in patients with detrusor overactivity who received permanent implants and satisfactory voiding in all implanted patients with urinary retention.
At present, the evaluation process consists of either PNE or tined lead testing. There is increasing evidence that two-stage evaluation with tined lead testing achieves better results by reducing the false-negative rate associated with the test procedure. Leong et al. 9 have recently shown in 82 patients over two years follow-up that the tined lead evaluation may be a more sensitive screening method than PNE in identifying patients eligible for a permanent implant. As would be expected, with the introduction of tined lead testing in our unit the number of PNE procedures has fallen. At the same time the conversion rate has increased from 45% in PNE group to 100% in tined lead group.
The fixation technique for the PNE lead has, however, caused some concern. There have been a number of instances where the effect of the device has diminished or disappeared completely within a short time of the procedure. It appears that this has been due to excessive mobility between the skin fixation of the electrode and the bony structure of the sacrum, particularly, in obese patients. The advantage of a PNE, however, is that lead is easily removed in the outpatient clinic whereas a tunnelled tined lead requires a general anaesthetic for removal. In view of this, we now proceed directly to a tined lead test in obese patients and in patients with non-obstructive urinary retention for whom a longer period of testing (3-4 weeks) is required. A PNE is, however, a simple and relatively inexpensive technique and, as such, continues to play an important role in the assessment process.
Our overall complication rate has been relatively low during the short follow-up period compared with longer follow-up studies. In a recent publication, Al-zahrani et al. 7 reported long-term results of sacral neuromodulation over 14 years period. Total explantation rate was 20.8% with the most common reason for the removal of the implant being lack of efficacy, although some patients also experienced painful stimulation and the radiation of stimulation to the leg. 5 There have been two health-care acquired infections, necessitating the removal of the tined lead electrode in one patient and the permanent implant in another. Outpatient visits have been higher than planned because of the large number of programming visits required by some patients. Moving the service to the New Victoria Ambulatory Care Hospital has allowed us to minimize inpatient stay and we now utilize a laminar flow theatre. These measures have minimized health-care associated infection.
Although this is a national service, geographical access remains an issue. Referrals are still patchy with some consultants referring large numbers of patients whereas there remain geographical ‘black holes’ with very few referrals for the population size. The distribution still remains skewed towards Greater Glasgow and Clyde (Table 1) presumably because of the transition from the West of Scotland Service which was subsumed into this service. We continue to present results at regional and national meetings to increase awareness of the service. We have reduced the number of visits to Glasgow to a minimum for remote patients but programming visits are required, usually a minimum of three times in the first year after implantation. When we reach a critical mass of patients we will set up regional programming clinics.
Safety, effectiveness and high patient satisfaction are key issues for patients who are considering this form of treatment and set it apart from alternative approaches. 10 However, the widespread adoption of SNS in the UK remains hampered by funding and cost issues (a patient episode including testing and permanent implant costs approximately £11,500). Our service is significantly limited by the number of funded permanent implants. Increasing awareness of the service will increase demand and, for the year 2011-2012, we estimate that there will be a requirement for at least 20 permanent implants.
Patient selection for permanent implant remains the corner stone of this therapy. This was supported by a recent Cochrane review which recommended that more research is needed on the best way to improve patient selection, carry out the implant, and to find reasons for failure. 11 Future research and technological developments are likely to advance the current practice, mainly in improving patient selection and reducing costs.
Conclusions
The results from the data collected during the first year since the Scottish SNS service has been established, have demonstrated that in selected patients SNS is a safe and effective procedure with the potential to improve quality of life.
It is most useful in patients with non-obstructive urinary retention, all of whom returned to spontaneous voiding following device implantation.
The limitation of funding for permanent implants inevitably impacts on the role of the technique as a management option for appropriate patients.