
Abstract
A significant proportion of patients presenting to hyperacute stroke units (HSUs) are diagnosed with non-stroke (NS). This study aimed to assess the rate and diagnoses of NS patients admitted to a HSU and the implications for clinical service provision. Admissions to the HSU at the Southern General Hospital, Glasgow, were retrospectively assessed (March 2007–September 2007). NS patients were identified by two parallel ascertainment methods and NS diagnosis was confirmed by case-note and discharge letter review. Of 375 presentations, 116 (31%) were due to NS. NS diagnosis was more likely for local referrals than from regional hospitals (41% versus 19%; P = 0.0002). Compared with stroke/transient ischaemic attack patients, NS patients were significantly younger, more likely to have an magnetic resonance imaging (MRI) scan and had a shorter length of hospital stay. Common NS diagnoses were migraine (22%), functional neurological disorder (14%), syncope (12%) and seizure (6%). NS patients who had an MRI scan were more likely to have a length of stay ≥2 days (75% versus 53%; P = 0.03). NS makes up one-third of acute stroke-like presentations with a high frequency of neurological conditions. NS patients tend to be younger and require significant investigation. The increased use of MRI and neurological services has implications for providing a hyperacute stroke service.
Introduction
A significant proportion of patients presenting to hyperacute stroke units (HSUs) are subsequently diagnosed with non-stroke (NS) diagnoses that mimic stroke. Some studies of in-hospital stroke-like presentations put the rate of NS at 5%; 1 however, studies of suspected stroke patients assessed in the hyperacute setting suggest the rate may be as high as 19-31%. 2 4 Rapid triage of suspected stroke patients to identify those eligible for thrombolysis may increase the rate of NS patients seen. This study aimed to assess the rate and diagnoses of NS patients admitted to an HSU and assess the implications on clinical and radiological service provision.
Methods
Admissions to the HSU at the Southern General Hospital, Glasgow, were assessed retrospectively over a seven-month period (March 2007–September 2007). Patients with a diagnosis of NS were identified by two methods: firstly, a stroke research nurse (YC) documented working diagnosis from a weekly clinical and radiological meeting at which all patients admitted to the HSU were discussed; secondly, cases of NS and stroke or transient ischaemic attack (TIA) were identified from the Scottish Stroke Care Audit database. Clinical diagnosis of NS was confirmed by case-note and hospital discharge letter review. If a discharge diagnosis of possible TIA or stroke was given by the treating stroke physician/neurologist with no alternative diagnosis offered, the diagnosis was categorized as stroke/TIA. If more than one possible discharge diagnosis was offered, the diagnosis was considered unclear and categorized as NS. A diagnosis of a functional neurological disorder relates to neurological symptoms not due to organic disease (e.g. functional hemiparesis, non-epileptic attacks and hemisensory symptoms). 5 7 Patients were referred to the HSU from local general practitioners, two local accident and emergency departments, wards within the same hospital or from seven regional hospitals within the west of Scotland that did not provide a thrombolysis service at the time of this study. Potential stroke patients were discussed with a neurology trainee who made the decision to admit the patient. Consultant-led care was delivered by a team of neurologists and elderly care physicians. Repeat admissions of the same patient within the time period were included. Patients admitted to the HSU were transferred to a combined acute stroke/rehabilitation unit within 24-48 hours. Comparison was made between patients with stroke/TIA and NS patients with regard to age, gender, use of cranial imaging (computerized tomography [CT] or magnetic resonance imaging [MRI]) and length of stay (LOS) in the hospital or HSU. This study was performed as an audit of service provision and, therefore, did not require ethical approval. Proportions were compared using the chi-square test and the t-test for parametric and the Mann-Whitney U test for non-parametric data. Significance was taken as P < 0.05.
Results
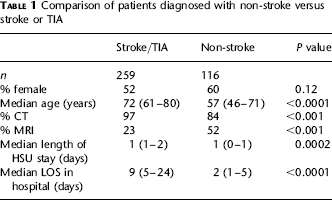
A total of 375 patient presentations to the HSU over the seven-month period were analysed. A total of 123 and 127 diagnoses of NS were identified by the first and second ascertainment methods, respectively, revised to 106 and 116 patients following review of case-notes and hospital discharge letters. This left a total of 116 NS presentations (31% of 375), including two repeat presentations. NS diagnosis was revised in a total of 27 patients from NS to stroke (n = 17) or TIA (n = 9) and one vertebral artery dissection. Data regarding route of referral was missing in 21% of patients. NS diagnosis was more likely for referrals from within the local hospital (i.e. from accident and emergency or ward, 42/102 [41%]) than from regional hospitals (22/118 [19%]; P = 0.0002). Of referred patients for consideration of thrombolysis from regional hospitals, the rate of NS was even lower (3/42 [7%]). The NS rate from primary care was 22/76 (29%). Compared with stroke/TIA patients, NS patients were significantly younger, were more likely to have an MRI scan, were less likely to have a CT scan and had a shorter LOS in hospital and the HSU (Table 1).
Comparison of patients diagnosed with non-stroke versus stroke or TIA
The main NS diagnoses (Table 2) were migraine/headache (22%), unclear (16%), functional (14%), neurocardiogenic syncope (12%), seizure (6%), vestibular (6%), infection (6%), intracranial malignancy (4%), Bell's palsy (4%) and other diagnoses (10%) (e.g. subdural haematoma, subarachnoid haemorrhage, radiculopathy, peripheral nerve lesion, multiple sclerosis, hypoglycaemic event, urinary retention, drug-induced movement disorder and pain syndrome). Patients with functional diagnosis, headache, vestibular disorder, Bell's palsy and seizure were significantly younger than the stroke/TIA group, whereas patients with a diagnosis of malignancy, unclear diagnosis or neurocardiogenic syncope had no age difference (Table 2). Of 16 patients presenting with functional neurological symptoms, specific diagnoses included functional hemiparesis (n = 8), non-epileptic attack disorder (n = 1), and predominantly panic and anxiety-related symptoms (n = 5; 1 with prior stroke). A higher proportion of NS patients were ≤45 years old compared with stroke/TIA patients (23% [27/116] versus 3% [10/269], respectively; P < 0.0001). There was a non-significant trend for longer LOS comparing NS patients who had an MRI scan with those who did not (median, 3 days; interquartile range, 1-5; n = 63 versus median, 1 day; interquartile range, 1-5; n = 57; P = 0.1). However, an in-hospital LOS of two days or more was more common in patients who had an MRI scan (75% versus 53%; P = 0.03). Forty percent of NS patients were discharged home from the HSU, 42% to stroke rehabilitation ward pending investigations and 8% were transferred to inpatient neurology care.
Main non-stroke diagnoses and age
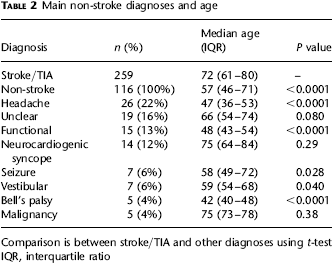
Comparison is between stroke/TIA and other diagnoses using t-test IQR, interquartile ratio
Discussion
Almost one-third of patients with suspected stroke left hospital with an NS diagnosis. NS patients were younger, had a shorter LOS in hospital and a higher rate of MRI imaging. Common NS diagnoses were migraine, functional presentations, syncope and seizure. NS referrals were more likely to come from local hospitals, perhaps due to ease of access, while peripheral hospitals referring patients predominantly for consideration of thrombolysis were less likely to refer NS patients. This latter observation may reflect the fact that proximity to a HSU encourages on-site referrals even when the referring physician is less confident of a diagnosis of stroke, while peripheral hospitals may be referring patients for consideration of thrombolysis and further clinical assessment that may require further neuroimaging. The high NS rate has implications for local resources. One study demonstrated an NS diagnosis rate of 25% in an acute stroke service, and the majority of NS diagnoses were conditions meriting urgent neurological assessment. 2 This provides a strong argument for the involvement of neurologists in assessing acute stroke-like presentations, as happens in many non-UK countries. Currently only some of the larger hospitals in Scotland can offer a neurological opinion on a daily basis to stroke units, although many hospitals will have a visiting neurologist on some weekdays. A prior study in Scotland also demonstrated an NS diagnosis rate of 31% in acute suspected stroke 2 and demonstrated several clinical predictors of stroke (e.g. an exact time of symptom onset, ability to classify stroke subtype and abnormal vascular findings). In contrast to our study ‘possible TIA or stroke’ was classified as NS. In our study the subgroup of possible TIA/stroke was small (n = 9), whereas in the aforementioned study 2 this group constituted 44/109 NS diagnoses. It is possible that the higher rate of MRI use may account for the small number of possible TIA/stroke in our study. 3 This study describes a relatively high rate of functional neurological NS presentation (14% of NS, but only 4% of the total population assessed). The minimal incidence of functional weakness has been estimated at 3.9/100,000 in the population of southeastern Scotland. 7 Such patients may require physiotherapy; if symptoms persist or recur, referral to psychology or liaison psychiatry may be indicated. 6
The role of MRI in aiding diagnosis merits mention. In one study only 3.5% of suspected stroke patients had normal imaging. 8 Of these patients the majority were still thought to have a clinical diagnosis of stroke, particularly lacunar stroke that may be missed by initial diffusion-weighted imaging MRI. 9 Current guidelines acknowledge the role of MRI in diagnosing TIA in up to 50% of patients. 10 In addition to its high sensitivity in identifying infarction, MRI also has a role in excluding stroke mimics given its high specificity in acute stroke. 10 In the current study patients diagnosed with NS had a high rate of MRI use. This had significant resource implications as patients tended to wait slightly longer in hospital, and MRI is not universally available acutely, particularly in the outpatient setting. The more prolonged LOS in NS patients having an MRI scan may be due to additional waiting time for MRI imaging or because diagnosis and management may take longer in some NS patients.
A number of decision-making tools have been developed to aid stroke diagnosis. The Recognition of Stroke in the Emergency Room (ROSIER) scale was developed to correctly identify acute stroke patients and exclude NS. 11 Although this scale has good negative and positive predictive values for stroke, it can misdiagnose lacunar and posterior circulation strokes as NS. 11 The ROSIER scale was validated in the same hospital setting from which it was developed and therefore may be less generalizable to different populations with different proportions of NS diagnoses. Prehospital scores may help reduce the NS admission rate; however, each scoring system has its limitations. For example, the Los Angeles prehospital stroke screen 12 and the Melbourne ambulance stroke screen 13 excludes patients <45 years old. A total of 27% (10/37) of patients aged ≤45 years in our study had a diagnosis of stroke or TIA, which may reflect the high burden of cardiovascular disease in the west of Scotland. Strategies to correctly identify stroke patients may reduce the NS diagnosis rate, with the potential risk of missing young patients with disabling stroke. In contrast, one study found no age difference between NS and stroke/TIA, which might be explained by lower rates of headache or migraine (2.8% versus 22%), and functional disorders (5.5% versus 14%) compared with the current study. 3 A prior study confirms, as in this study, that the most common stroke mimics seen in thrombolysed patients (seizure, conversion disorder, migraine) are younger than the average stroke patient. 14 As noted even those patients subsequently treated with thrombolysis for acute stroke have a significant misdiagnosis rate. One recent study of a centre's experience with stroke thrombolysis noted 14% of treated patients had a discharge diagnosis of NS. 15 None of the patients appeared to have an adverse outcome following thrombolysis with the main diagnoses being seizure, complicated migraine and conversion disorder, in concurrence with another study. 14
Conclusion
NS makes up a significant proportion of acute stroke-like presentations. This subgroup of patients tends to be younger than the average stroke patient and exhibit a range of diagnoses more typically treated by neurologists than general physicians. The role of neurology services and the high rate of MRI imaging have resource implications for those providing an acute stroke service.