The expected duration of initial antiparkinson monotherapy before the need for supplementation is not clearly defined for routine practice. The aim of this study was to define the length of l-dopa (L-3, 4-dihydrophenylalanine) and dopamine agonist monotherapy. The duration of monotherapy and discontinuation rates were investigated in a natural observational setting by plotting Kaplan–Meier survival curves. Out of 345 patients, 180 (52.2%) received l-dopa and 165 (47.8%) received a dopamine agonist as initial monotherapy. Half of the patients starting l-dopa received supplementary therapy within 3.6 years (95% confidence interval, 3.2-4.6), significantly longer than for dopamine agonist monotherapy (half required a second agent at 2.3 years [2.0-2.9]; P = 0.00017). Discontinuation of l-dopa therapy was 1%. Dopamine agonists were stopped (due to side-effects like impulse control disorders [6%], somnolence [4%] and light-headedness [3%]) in 20% over four years. The duration and tolerability of l-dopa and dopamine agonists as initial Parkinson's disease monotherapy are defined in this study; this may form part of the information exchange with patients.
l-Dopa (L-3, 4-dihydrophenylalanine) or dopamine agonists are a frequent initial drug choice in the treatment of Parkinson's disease (PD).1 Dopamine agonists delay the onset of l-dopa–related motor complications,2,3 but cause more neuropsychiatric side-effects such as hallucinations and impulse control disorders.4,5 Patients frequently enquire about the duration and extent of benefit to be expected from their initial antiparkinson agent before supplementary treatment will be needed. Some information on this topic is available from comparative monotherapy trials of l-dopa and dopamine agonists.2 The restrictive entry criteria for clinical trials reduces the generalizability of these results. Naturalistic studies are therefore of interest as they encompass a more varied and clinically heterogeneous population.6 Such studies of routine clinical practice are generally smaller than recent clinical trials and include cases at all disease stages, so the number of patients taking monotherapy is typically fewer than 100.711 We report here the observations in a large clinical series of early stage PD patients. Our aims were to define the duration of l-dopa monotherapy compared with dopamine agonists before adjunctive treatment in a naturalistic clinic setting and to define adverse events and associated discontinuation rates, and contrast the findings with those in clinical trials.
Methods
Patients were identified from a review of database and paper records in three linked movement disorder clinics in the west of Scotland. The clinics included regional neurology and joint neurology and medicine for the elderly services. Routine outpatient attendances occured every six months and were supplemented by interim nurse specialist and medical telephone advice and additional visits, typically related to adverse events or inadequate efficacy. Domperidone is not co-prescribed routinely, but patients and their primary care physicians are specifically guided to add these should nausea or light-headedness occur. Inclusion criteria for the study were: diagnosis of PD by a movement disorder specialist based on UK Brain Bank criteria and presynaptic dopamine transporter imaging in cases of diagnostic uncertainty; that patients be taking an oral non-ergot dopamine agonist (ropinirole or pramipexole) or l-dopa-based treatment as initial monotherapy; and the availability of follow-up data for a minimum of one year after starting monotherapy. Patients were excluded if the diagnosis was amended to an alternative degenerative Parkinsonian syndrome. Other antiparkinson agents (e.g. monoamine oxidase B inhibitors) introduced as initial monotherapy were not studied as these are used much less commonly in our service. Concomitant or prior medication with any antiparkinsonian agent was not allowed at baseline. The decision between dopamine agonist and l-dopa as initial monotherapy was made by one of five movement disorder clinicians on an individual case basis, as was the decision to add second-line therapy. For patients started on l-dopa or dopamine agonist as monotherapy, the time to addition of a second agent was calculated. The time to discontinuation of initial l-dopa or dopamine agonist treatment was also calculated. Patients could be supplemented with a second agent at this point.
Results were charted by Kaplan–Meier survival analysis using GraphPad Prism (version 4.03; GraphPad Software, Inc., La Jolla, CA, USA). l-dopa equivalent units (LEU) were calculated by standard formula.12
Results
Of 345 patients, l-dopa was the initial monotherapy in 180 cases (52.2%), while dopamine agonists were the initial monotherapy in 165 (47.8%) – either ropinirole (n = 116; 33.6%) or pramipexole (n = 49; 14.2%). l-dopa-treated patients were 74.4 years old (interquartile range [IQR], 69.5-79.0), which was about 10 years more than the dopamine agonist group (63.6; IQR, 56.1-69.0) (Table 1).
Demographics and duration and dosage of antiParkinson therapy in 345 Parkinson's disease patients
Maximum dose in patients stopping dopamine agonists
8 (3-18) mg
0.8 (0.5-2.4) mg
–
Maximum dose in patients continuing dopamine agonists
12 (9-18) mg
2.1 (1.6-3.2) mg
–
Age at diagnosis in patients stopping dopamine agonists
63.0 (55.6-70.4)
71.4 (68.1-77.3)
69.0 (60.0-72.7)
Age at diagnosis in patients continuing dopamine agonists
62.0 (55.1-66.0)
64.3 (58.0-67.0)
62.3 (56.4-66.5)
LEU, l-dopa equivalent units
Figures are numbers (%) or median (interquartile range)
L-dopa dose before second agent added significantly higher than dopamine agonist dose (P = 0.0001)
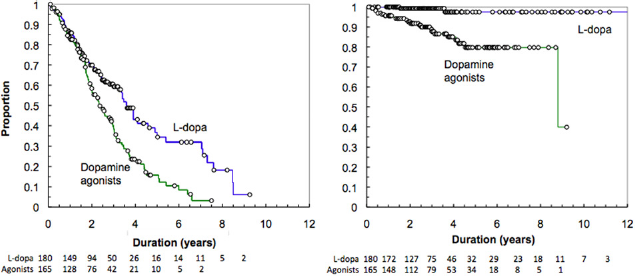
More patients starting dopamine agonists required a second agent than patients starting l-dopa. While survival on initial monotherapy was similar for l-dopa and dopamine agonists for around 1.8 years, it diverged thereafter, becoming longer for l-dopa than dopamine agonists. Half of patients starting L-dopa received supplementary therapy by 3.6 years (confidence interval [CI], 3.2-4.6), which was significantly longer than the duration of dopamine agonist monotherapy (2.3 years; CI, 2.0-2.9; P = 0.00017, log rank) (Figure 1, left panel).
Kaplan–Meier curves for initial monotherapy in 345 Parkinson's disease patients. Left panel: Time to introduction of a second antiparkinson agent according to baseline monotherapy (l-dopa or dopamine agonist). Right panel: Time to discontinuation of initial monotherapy. Circles represent individual cases; numbers below the graphs indicate patients remaining ‘at risk’ each year
Discontinuation of l-dopa treatment was rare, while about 20% of dopamine agonist treated patients discontinued, mostly within the first four years; thereafter patient numbers on dopamine agonist treatment remained stable (log rank, P < 0.0001) (Figure 1, right panel).
Of the l-dopa patients requiring a second agent, entacapone was used in 64 (76%), dopamine agonists in 13 (15%), amantadine in three (4%) and rasagiline in two (2%) cases. For initial dopamine agonist therapy the second agent was l-dopa in 110 (89%) and selegiline in 13 (11%).
The reason for therapy supplementation was documented in the 82 l-dopa cases as limiting the dose of l-dopa (usually 400 mg/day) in 47 (57%), lack of efficacy in 39 (48%), side-effects in 11 (13%), dyskinesia in 8 (10%) and other in 4 (5%). In the 123 dopamine agonist patients in whom supplementation was given, reasons were: side-effects in 60 (49%), lack of efficacy in 38 (31%) and reaching maximum recommended dose in 23 (19%); some patients had more than one reason.
Of 165 patients starting a dopamine agonist as monotherapy, 31 (19%) stopped the first agonist. In 15 (9%) of these an alternative dopamine agonist was introduced; this was maintained in 10 (66.6%) of those cases.
Side-effects were significantly more common on dopamine agonists than l-dopa overall.
Impulse control disorders occurred in 11.7% of patients taking dopamine agonist monotherapy (pathological gambling 7.6%, hypersexuality 3.6%, excessive eating 3.3%, compulsive shopping 1.1%, others 3.9% [e.g. completing puzzles, computing, vacuuming, door locking, checking the weather forecast]) and were most common reasons (6%) for stopping dopamine agonist treatment, followed by somnolence (4.2%), hallucinations (3.6%) and light-headedness (3%).
Discussion
Our study defines discontinuation rates and the duration of dopamine agonist and l-dopa monotherapy before the addition of a second antiparkinsonian agent in a natural clinical setting, providing information that may be used in discussion with PD patients and their families.1 Previous observational studies have largely focused on discontinuation rates for dopamine agonists introduced as a supplement to l-dopa, rather than requirements after starting monotherapy.7,8,11,13 We acknowledge that our study addresses only one component of the treatment decision pathway, which varies across different centres, and that we did not capture data relating for example to the initial use of rasagiline or alternative treatments. While some data on the duration of monotherapy is available from clinical trials, nearly all such studies allowed open-label l-dopa as a supplement, or monoamine oxidase B inhibitors or amantadine as concomitant medication,3,14–16 and none one of the studies reported survival analysis. Maintenance of dopamine agonist monotherapy varies: 83% at eight months,17 44% at 12 months,14 86% at two years15 and 36-52% at three years,16,18 which probably reflects variation in study design and setting. While accepting that the dose at which a second agent is added to initial monotherapy in PD is subject to individual consideration in daily clinical practice and may differ across centres, our survival analysis results are in keeping with the clinical trial observations for dopamine agonists and give an added perspective relative to l-dopa. Another difference is the lower doses used in clinical practice compared with clinical trials, in which a maximally tolerated dose of a single agent is often encouraged before supplementary therapy. In our study, l-dopa patients received supplementary therapy, mainly entacapone, at a median dose of 400 mg l-dopa per day. In clinical trials, l-dopa doses reached a mean of 753 mg (including open-label supplementation),3 while ropinirole-treated patients in two clinical trials were supplemented at a mean dose of 16.5 and 12.7 mg before adding open-label l-dopa, both higher than the 9 mg dose at which supplementation was given in our series.3,16 Extended open-label observational studies after completion of double-blind comparative studies of l-dopa and dopamine agonists reported maintainence of pramipexole in around 80% at six years19 and 90% between years 5 and 10 for ropinirole,13 similar to those in the present study. However, these higher maintenance rates for dopamine agonists have not been reported in clinical trials, in which discontinuation rates are typically 15-20% at two years and 40% at 3-5 years.3,16,17,20–22 In our study dopamine agonist discontinuation and supplementation of initial monotherapy were both largely driven by adverse events, in particular impulse control disorders, which were recorded at rates similar to those in a recent cross-sectional study.23
In conclusion, this study provides practical comparative information about drug administration with either L-dopa or dopamine agonists as monotherapy in daily clinical practice.
Footnotes
Acknowledgements
The authors thank Angela O'Donnell, Elaine Thomson, Elaine Tyrrell, Tracy Murphy, Margaret Mitchell, Anne McWilliams, Rosemary Tracey, Margaret Crawford, Elizabeth Jackson and Anna McMillan for specialist nursing and secretarial and organizational support.
Financial disclosures: TN, MD, GP and KAG have no financial disclosures. EJN received honoraria from Eisai (lectures) and UCB (travel grant). MS received travel grants from UCB and Orion. PO received honoraria (advisory boards/lectures) from Boehringer-Ingelheim, Solvay/Abbott, Cephalon, GSK and UCB. GJM received honoraria (advisory boards) from Boehringer-Ingelheim, GSK, Teva and Solvay; grants/research support from Boehringer-Ingelheim and UCB; and travel grants from Boehringer-Ingelheim, Orion, GSK and Solvay. DGG received consultancy fees from Vectura; honoraria (lectures) from Boehringer-Ingelheim; grants/research support from Eisai; and on the advisory boards of GSK and Cephalon.
References
1.
GrossetDG, MacpheeGJA, NairnM.Diagnosis and pharmacological management of Parkinson's disease: summary of SIGN guidelines.BMJ2010; 340: b5614.
2.
WattsRL, LyonsKE, PahwaR.Onset of dyskinesia with adjunct ropinorol prolonged-released or additional levodopa in early Parkinson's disease.Mod Disord2010; 25: 858–66.
3.
RascolO, BrooksDJ, KorczynAD, for the 056 Study Group. A five-year study of the incidence of dyskinesia in patients with early Parkinson's disease who were treated with ropinirole or levodopa.N Engl J Med2000; 342: 1484–91.
4.
BiglanKM, HollowayRG, McDermotMP, RichardIH Parkinson Study Group CALM-PD Investigators. Risk factors for somnolence, edema, and hallucinations in early Parkinson disease.Neurology2007; 69: 187–95.
5.
GrossetKA, MacpheeG, PalG.Problematic gambling on dopamine agonists: not such a rarity.Mov Disord2006; 21: 2206–8.
6.
LeufkensHG, UrquartJ.Variability in patterns of drug usage.J Pharm Pharmacol1994; 46: 433–7.
7.
ArbouwME, MovigKL, GuchejaarHJ.Discontinuation of ropinirole and pramipexole in patients with Parkinson's disease: clinical practice versus clinical trials.Eur J Clin Pharmacol2008; 64: 1021–6.
8.
ArbouwME, MovigKL, EgbertsTC.Clinical and pharmacogenetic determinants for the discontinuation of non-ergoline dopamine agonists in Parkinson's disease.Eur J Clin Pharmacol2009; 65: 1245–51.
9.
ShulmanL, MinagarA, RabinsteinA, WeinerW.The use of dopamine agonists in very elderly patients with Parkinson's disease.Mov Disord2000; 4: 664–8.
10.
AltamuraAC, MauriMC, De NovellisF, PercudaniM, VampiniV.Residual neuroleptic-induced Parkinsonian symptoms in schizophrenia. a naturalistic study with orphenadrine.Pharmacopsychiatry1989; 22: 246–9.
11.
ValldeoriolaF, CobaledacS, LahuertacJ.A multicentre retrospective study of the clinical use of ropinirole in the treatment of Parkinson's disease: the ROPI-PARK study.Clin Neurol Neurosurg2009; 111: 742–7.
12.
ParkinSG, GregoryRP, ScottR.Unilateral and bilateral pallidotomy for idiopathic Parkinson's disease: a case series of 115 patients.Mov Disord2002; 17: 682–92.
13.
HauserRA, RascolO, KorczynAD.Ten-year follow-up of Parkinson's disease patients randomized to initial therapy with ropinirole or levodopa.Mov Disord2007; 22: 2409–17.
14.
SethiD, O'BrienCF, HammerstadJP.Ropinirole for the treatment of early Parkinson's disease. A 12-month experience.Arch Neurol1998; 55: 1211–6.
15.
WhoneAL, WattsRL, StoesslAJ.Slower progression of Parkinson's disease with ropinirole versus levodopa: the REAL-PET study.Ann Neurol2003; 54: 93–101.
16.
KorczynAD, BruntER, LarsenJP, NagyZ, PoeweWH, RuggieriS.A 3 year randomized trial of ropinirole and bromocriptine in early Parkinson's disease.Neurology1999; 53: 364–70.
17.
ShannonKM, BennettJP, FriedmanJH.Efficacy of pramipexole, a novel dopamine agonist, as monotherapy in mild to moderate Parkinson's disease.Neurology1997; 49: 724–8.
18.
OertelW, WoltersE, SampaioC.Pergolide versus levodopa monotherapy in early Parkinson's disease patients: the PELMOPET study.Mov Disord2006; 21: 343–53.
19.
Parkinson Study Group, CALM Cohort Investigators. Long-term effect of initiating pramipexole vs levodopa in early Parkinson disease.Arch Neurol2009; 66: 563–70.
20.
HollowayRG, ShoulsonI, FahnS.Pramipexole vs levodopa as initial treatment for Parkinson disease: a 4-year randomized controlled trial.Arch Neurol2004; 61: 1044–53.
21.
BrooksDJ, AbbottRJ, LeesAJ.A placebo-controlled evaluation of ropinirole, a novel D2 agonist, as sole dopaminergic therapy in Parkinson's disease.Clin Neuropharmacol1998; 21: 101–7.
22.
HubbleJP, KollerWC, CutlerNR.Pramipexole in patients with early Parkinson's disease.Clin Neuropharmacol1995; 18: 338–47.
23.
WeintraubD, KoesterJ, PotenzaMN.Impulse control disorders in Parkinson's disease: a cross-sectional study of 3090 patients.Arch Neurol2010; 67: 589–95.