
Abstract
The study was undertaken to determine the value of fine needle aspiration cytology (FNAC) in the investigation of breast lumps at the University Teaching Hospital (UTH) in Lusaka, Zambia. This technique, which has been shown to be cheap, simple and accurate has not been in common use at this institution. FNAC and open biopsy (OB) were performed on 56 patients who presented with a breast lump and the results compared, in order to determine the accuracy of FNAC. FNAC was found to have a sensitivity of 72% and specificity of 100%. This level of accuracy compares favourably with the quality assurance criteria set for breast FNAC by the Royal College of Pathologists in the British National Health Service (NHS).
Introduction
The technique of fine needle aspiration cytology (FNAC) was first described by Kun in 1847. 1 It was introduced into clinical practice by Ellis and Martin in the 1930s. 2 In 1989 the Royal College of Pathologists produced guidelines for the use of FNAC in the diagnosis of breast lumps in the National Health Service (NHS) in the United Kingdom (UK). 3 In Africa, the technique has not been widely used, inspite of being cheap, simple and accurate. In 1991 Mr Yusuf Kodwavalva, in the third Rahima Dawood lecture to the Association of Surgeons of East and Central Africa, endorsed its use in resource-poor countries. 4
University Teaching Hospital (UTH), Lusaka, is the main referral hospital in Zambia, with a catchment area of over 10 million people. Some cytology reporting has been done, mainly of cervical smears and FNAC of lymph nodes. 5
In Zambia breast cancer is the second commonest cancer in women after cancer of the cervix. 6 It is on the increase in Africa, where it presents a decade earlier than in developed countries and runs an aggressive course. 7
UTH does not have mammographic facilities. Although mammography is available outside the public health system, the cost of approximately 100 US$ is beyond the means of the majority of patients from low socioeconomic groups. Moreover, mammography is less sensitive in the younger women commonly presenting with breast cancer in our society, because of the greater density of their breast tissue. 8,9
At UTH clinical assessment, ultrasound and open biopsy (OB) are used to diagnose breast lumps. However, the consent rate for OB is low, except in patients with stage 3 and 4 disease, i.e. with obvious debilitating symptoms. Therefore the aim of this study to assess whether FNAC can be used as an accurate and more acceptable alternative to OB in the diagnosis of breast lumps.
Methods
A dedicated outpatient clinic was started at UTH, where all women presenting with breast lumps were seen. Only newly presenting patients with breast lumps were included in the study. A detailed capture sheet was completed for each patient by the researchers until their final discharge. FNAC was done at the first visit and the patient reviewed two weeks later and given the results. Those who consented then had OB of the lump on the next available theatre list, under local or general anaesthesia, depending on the size of the lump.
The technique used for FNAC was as described by Parsons. 7 No anaesthesia was used. The lump was held between thumb and index finger. A blue 21 gauge needle was used for superficial lumps and a green 23 gauge needle for deeper ones. The needle was attached to a 10 mL syringe and inserted into the lump. Suction pressure was applied by withdrawing the syringe plunger to the 10 mL mark. Three to four passes were made into the substance of the lump, keeping the needle within the breast at all times. This allowed detachment of cells, which were suctioned into the needle hub. The needle was withdrawn and the aspirate expressed and thinly spread on to a clean dry glass slide, which was air dried and stained with a Giemsa stain. A minimum of two slides were prepared for each patient.
The method of staining was as follows: the slides were fixed in alcohol for 5 minutes and then stained in Giemsa stock and 45 mL pH 7.0 water for 1 hour. They were differentiated in 0.2% acetic acid and rinsed in tap water. A cover slip was then fixed with DPX (the synthetic mounting medium distrene, plasticizer and xylene).
The results were reported by a consultant pathologist with special training in breast cytology using the 5 scale reporting system of the UK Royal College of Pathologists: C1 acellular, C2 benign, C3 likely benign but some atypia, C4 suspicious of malignancy, C5 malignant. 3 The reporting of the histopathology was done independently of the cytology with the pathologists blinded to the cytology results.
The level of accuracy of FNAC in diagnosing malignant breast lumps was determined from the sensitivity and specificity. The sensitivity was defined as the number of C5 FNAC results over the total number found to be malignant at OB. Specificity was the number of C2 FNAC results over the number of those found to be benign at OB.
Results
A total of 97 women were included in the study. The average age was 26 (range 13–51). All patients agreed to have FNAC. Only 56 agreed to have an OB, which gives it an acceptance rate of 58%, compared with 100% for FNAC.
The FNAC and OB results are shown in Table 1. FNAC was found to be 72% sensitive (18/25) and 94% specific (29/31) in the diagnosis of breast cancer.
Fine needle aspiration cytology and open biopsy results
Discussion
In Zambia diagnostic tools for breast lumps are limited. We have at our disposal clinical assessment and, more recently, ultrasound. The WHO does not recommend the use of mammography in developing countries because of the cost of introduction and its limited usefulness because of the young average age of patients presenting with breast lumps. 10 In order to get a pathological diagnosis we have traditionally had to rely on OB. This study shows that this is only acceptable to 58% of patients.
The place of FNAC in the diagnosis of breast cancer is well established. In 1989, the UK Royal College of Pathologists produced guidelines for its use in the NHS and these have subsequently been updated, most recently in 2001. 11 In a summary of 12 studies and a total of 13,286 patients, de Ferietas found the sensitivity and specificity of breast FNAC to range between 87 and 99%. 12
Our study shows FNAC to be 100% acceptable to our patients. Moreover the cost of FNAC is 20 US$, compared with 100 US$ for OB. Our 72% sensitivity and 100% specificity rates are within those recommended by the Royal College of Pathologists for quality assurance (>70% and >65%, respectively). Inadequate samples (i.e. C1 results) accounted for 7% of our cases, well within the 15% recommended.
As a result of this study, the management of breast lumps has changed at UTH. As no C2 result was shown to be malignant at OB, we manage a C2 aspirate purely according to lump size and patient preference. Lumps are excised if they are greater than 4 cm in diameter or at the patient's request. Those under 4 cm are followed up in the outpatient clinic with clinical assessment and ultrasound. It is clear that C1, 3 and 4 FNAC results must be regarded as inconclusive and in these cases (12.5% of patients) we proceed to diagnostic OB. Indeed, if equivocal C1, 3 and 4 cases are disregarded, FNAC becomes 100% sensitive as well as 100% specific for malignancy. Although all our C5 FNAC results corresponded with malignancy at OB, we feel that the number of cases (18) is not yet high enough for us to dispense with OB prior to definitive surgery in these patients. We hope to be able to change this in due course.
We have shown that FNAC can be used accurately and reliably in the developing world to assess breast lumps. Moreover, it is cheap and acceptable to patients. The wider use of FNAC in environments such as ours overcomes the disadvantages of other diagnostic modalities and improves the efficiency and speed of diagnosis of breast disease.
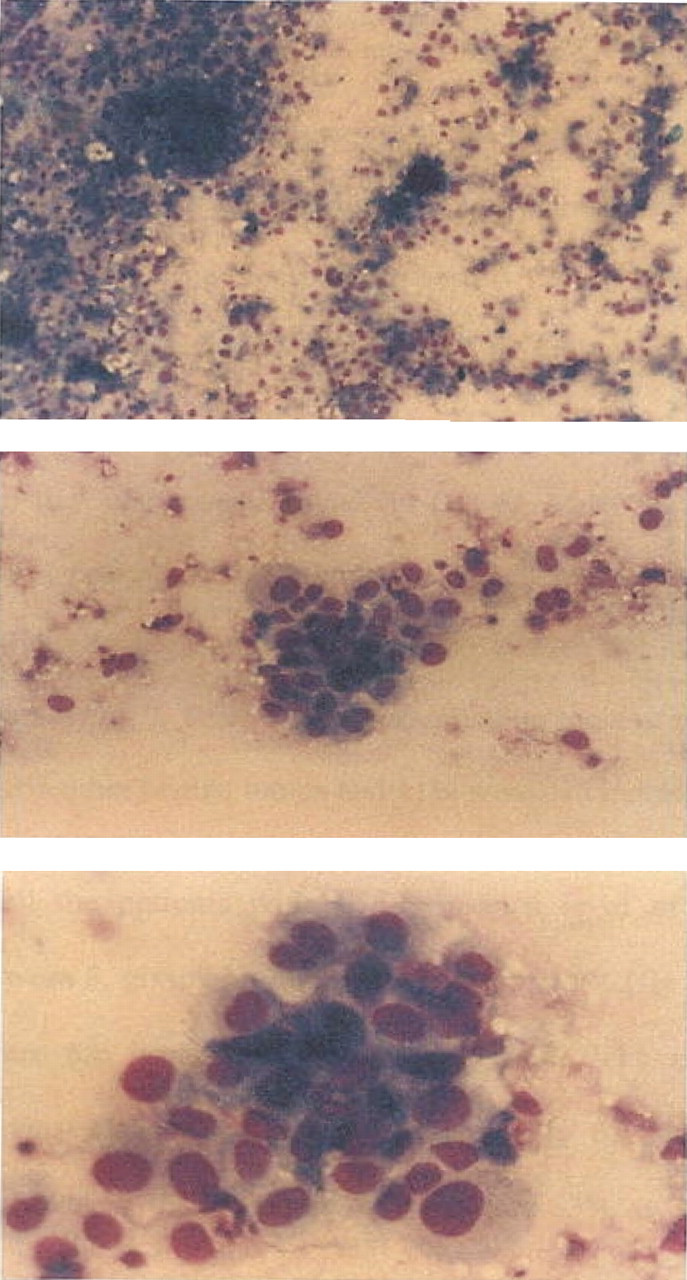
Benign cytology stained with Giemsa stain, the cells are viewed at ×4, ×10 and ×20 magnification. The cells are of two types, they are clumped, very cellular and cohesive. The nucleus is dominant (Photograph of Breast Cytology Cells at University Teaching Hospital Lusaka Medical Illustration department credit Dr Kasonde Bowa) Fine needle aspiration cytology of a malignant cytology stained with Giesma at increasing magnification of ×4, ×10 and ×20. The cells are large independent, the nucleus is active with prominent nucleoli, no bare cells are seen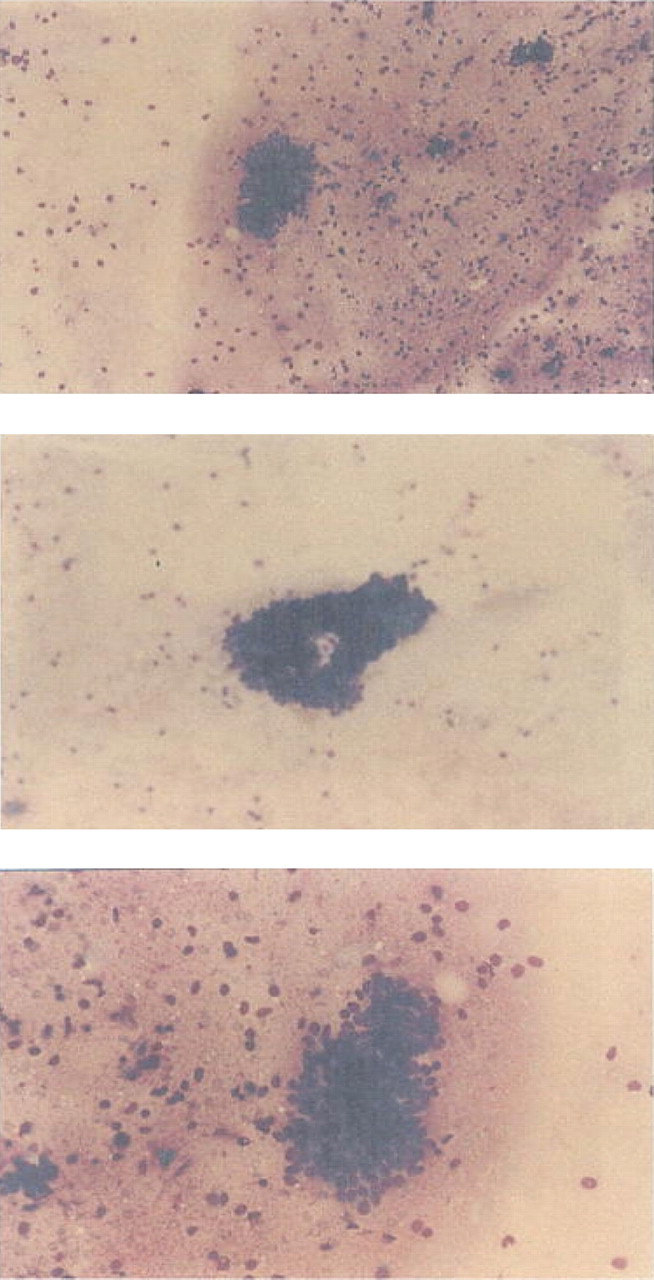
Footnotes
Award
This study was awarded the Belgium Prize for Developmental Research, 2000.