
Abstract
This retrospective study was performed in two university hospitals between January 2002 and 2006. Ninety-nine brucellosis patients were included in the study. These patients were classified as acute (91), chronic (4) and relapse (4) according to their clinical presentations and serological tests. Brucella bacteria were isolated in the blood of 17 (17.2%) cases. The most frequent symptom and clinical sign was fever. The osteoarticular complications were found in 17 patients (17.2%). Four of them were complicated with epidural abscess the same time. Two (2.2%) had meningitis, two (2.2%) had epididymoorchitis, three (3.3%) had skin rashes and one (1.1%) had hepatitis. Three of the acute brucellosis patients were pregnant. Rifampin and doxycycline combination therapy had been administered to most of the patients with acute and relapse brucellosis. However, complicated and chronic brucellosis cases were given different treatment combinations. This study reviews brucellosis therapy choices.
Introduction
Brucellosis, which is a zoonosis with worldwide distribution, is a systemic infection. It is still an important public health problem throughout the world, but principally, in the Mediterranean region included some parts of Turkey, the Arabic Peninsula and India where it is endemic. It is responsible for enormous economic losses and considerable human morbidity in these endemic areas. The diagnosis is difficult as brucellosis can affect multiple organs and systems and there are different clinical symptoms and findings. In complicated cases, controversy still reigns over the optimal treatment regimens and the duration of treatment.1,2
The aim of this study is to present the epidemiological features and the clinical spectrum of brucellosis and to discuss the characteristics of brucellosis therapy in the mid-Anatolian region of Turkey, a moderately endemic area for brucellosis.
Materials and methods
The study was conducted retrospectively. Patients who were hospitalized in two university hospital in mid-Anatolia between January 2002 and 2006 were included in the study. They were evaluated by age, sex, residence, possible modes of transmission, symptoms, signs, laboratory findings, clinical forms (acute, chronic and relapse), complications, treatment regimens and duration of treatment.
The diagnosis of brucellosis was based on clinical signs and symptoms, serological methods (including the Rose-Bengal slide agglutination test and the Wright tube agglutination test) and the isolation of Brucella species in blood cultures (Bactec). The positive Rose-Bengal test was absolutely confirmed with Wright test. A titre of 1:160 or higher or a titre lower than 1:160 showing a four-fold increase within two weeks were considered positive in the Wright test. Serial dilutions were extended to 1:2560, in order to avoid the prozone phenomenon.
Cases were classified as acute, chronic and relapsing brucellosis. Subjects with clinical manifestations of eight weeks or less were considered acute, those persisting for more than 48 weeks were considered chronic. Patients with recurring symptoms 48 weeks after the initial treatment and positive serologic tests or positive blood or body fluid cultures were reported as relapsing brucellosis. Complications were evaluated by physical examination, radiological examinations and cerebrospinal fluid tests. Treatment regimens were assessed for each patient and publications on the treatment of brucellosis were reviewed.
The criteria for complete recovery were normal physical examination findings, normal erythrocyte sedimentation rate (ESR) and C reactive protein (CRP) levels, a negative Rose Bengal test and at least a two-fold decrease in the Wright agglutination test titre. Those who completed the treatment regimen and the 18-month post-treatment follow-up period were assessed in terms of relapse.
Result
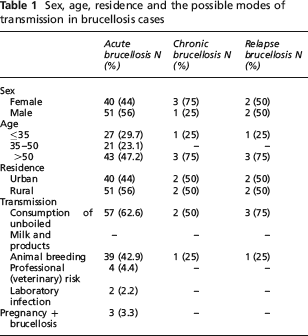
Ninety-nine cases with brucellosis were evaluated. Of these, 91 (91.9%) were recorded as acute, for (4.05%) as chronic and four (4.05%) as relapsing brucellosis. Sixty-two (62.6%) had a history of the consumption of raw milk and milk products, 41 (41.4%) had contact with breeding animals, three (3%) had occupational contact with breeding animals and two (2%) had laboratory infections. The mode of transmission was not clear in 27 (27.3%) patients. Three patients with acute brucellosis (3.3%) were pregnant. Sex and age distributions, the residence of the patients and the possible modes of transmission of the disease are presented in Table 1.
Sex, age, residence and the possible modes of transmission in brucellosis cases
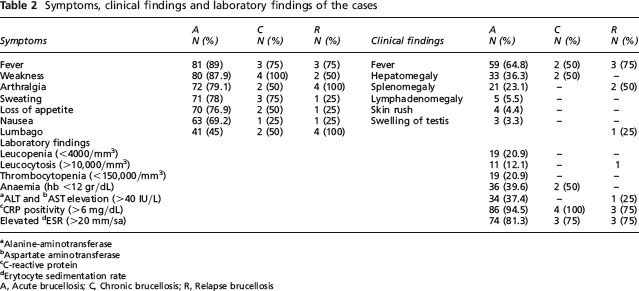
The most frequent symptom and clinical sign was fever. Table 2 shows those symptoms and physical examination findings.
Symptoms, clinical findings and laboratory findings of the cases
Alanine-aminotransferase
Aspartate aminotransferase
C-reactive protein
Erytocyte sedimentation rate
A, Acute brucellosis; C, Chronic brucellosis; R, Relapse brucellosis
While Brucella species were isolated from blood cultures in 17 cases (17.2%), isolation was not possible in 82 patients (82.8%). The Rose Bengal and the Wright tests were positive in all patients. Table 2 shows the additional laboratory tests used to support the presumptive diagnosis.
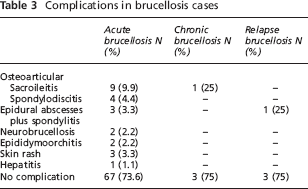
Three patients (3.3%) with brucellosis were pregnant. Overall, the most common complication site was the osteoarticular system. Complications according to clinical types are listed in Table 3.
Complications in brucellosis cases
While the most common treatment regimen for acute and relapsing cases was rifampin + doxycycline, the rifampin (R) + doxycycline (D) + ciprofloxacin (CP) regimen was used more often for chronic cases. Treatment regimens and the duration of treatments are shown in Table 4. All patients were cured except one acute case complicated with neurobrucellosis who died at week 3 of treatment.
Treatment regimens and durations in brucellosis cases

Cases with complicated epidural abscess
Cases with neurobrucellosis. One of them died at third week of the treatment
Cases with osteoarticular complications
Pregnant cases
R, Rifampin; D, Doxycycline; CAX, Ceftriaxone; STR, Streptomycin; CP, Ciprofloxacin
The post-treatment 18-month follow-up was completed in 30 cases with acute brucellosis, four with epidural abscess, one with neurobrucellosis, 10 with osteoarticular complications, three with relapsing disease and two who were pregnant. No patient showed relapse.
Discussion
Brucellosis is a disease seen throughout Turkey, especially in the mid-Anatolia region, and notification of the disease is mandatory. In 2001, a total of 15,510 brucellosis cases were reported throughout the country. 3 Of these, 682 (4.4%) were reported from areas where the two universities in which this study was conducted are located. 4 Stockbreeding is the main mode of making a living in these regions and the consumption of milk and milk products is frequent in the towns and villages. The major mode of transmission in our study was the consumption of contaminated milk and milk products. Another important mode of transmission was via occupational accidents among animal breeders, veterinarians, butchers and microbiologists.5,6 The possible sites of entrance for the bacteria in such transmission are the skin and the conjunctiva. 5 In case series reported in Turkey, the most common most of transmission is the consumption of milk and products.7,8 This can probably be explained by the fact that boiling is the most widely used method of disinfecting milk in mid-Anatolia. Pasteurized milk is not common in this region and milk products containing contaminated milk are sold and consumed extensively throughout the country.
Brucellosis may involve many organs. It may have an acute, subacute or chronic course. The disease may relapse after cessation of treatment regardless of antibiotic resistance. 1 Hence, patients present with many different symptoms. Fever, sweats, fatigue, low back pain, joint pain, myalgia and loss of appetite are the most common symptoms. 1 In our study, the most common symptom in acute, chronic and relapsing cases was fever.
Blood culture positivity in brucellosis ranges between 15 and 70%.1,7 Waiting for the culture results may delay the initiation of treatment. Thus, titres of 1:160 and higher in the standard tube agglutination test are considered to be diagnostic.1,9 The diagnosis was based on isolation of the bacteria in blood cultures in 18.7% of the cases in our study. CRP was positive in 94.5% of the acute cases, 100% of the chronic cases and in 75% of the relapsing cases. CRP became negative after treatment in all patients. CRP, an acute phase reactant synthesized in hepatocytes, increases in acute brucellosis cases and returns to normal levels after the treatment. 10 CRP may be used to confirm the diagnosis and to monitor the response to treatment in culture-negative patients diagnosed with serology. The results obtained through monitoring CRP levels in our study confirm this.
The most common complications of human brucellosis are osteoarticular complications which are reported to range between 20 and 85%.1,11 We identified 17.2% osteoarticular complication in this study. Our discordant results, i.e. low ratios, may have been caused by our using sensitive radiological techniques to demonstrate the presence of osteoarticular problems. The rates of other complications in our study were found to be similar to that reported in the literature.1,5,12
As brucella bacteria are facultative intracellular parasites, single and short-term drug therapy causes relapses. It is therefore necessary to use at least two drugs for a long time period. The World Health Organization (WHO) recommends 2 × 100 mg/day D and 15 mg/day/kg R combination therapy for six weeks. 12 This therapy protocol had been administered to most of the patients with acute and relapse brucellosis among in our cases. The cases complicated with epididymoorchitis, skin rash or hepatitis were treated by D + R therapy combination. Four patients received R + CP. All of them were cured within six weeks. Although the standard regimen recommended by WHO is D and R combination, in recent years both in vitro and in vivo fluoroquinolones have been shown to be effective in the treatment of brucellosis.13–16 The literature recommends that fluoroquinolones be used in combination with R or D for the treatment of acute brucellosis as an alternative to the R and D combination, if needed. However, these agents should not be used as monotherapy for the treatment of brucellosis. 16
Paraspinal abscess accompanies spondylitis in 10–20% of brucellosis patients. However, epidural abscess accompanying spondylitis is very rare.17,18 Epidural abscess was present in addition to spondylitis in one relapsing and three acute brucellosis cases in our study (4%). Interestingly, these patients responded to R + D treatment without any need for surgical intervention and no relapses were recorded during the 18-month follow-up period. The recommendation for cases with spondylitis accompanied by epidural abscess is to prolong the duration of therapy without surgical intervention unless spinal chord compression is present. 19 Reports suggest that treatment regimens including streptomycin (STR) would be more beneficial in brucellosis cases complicated with spondylitis and epidural abscess. 1 Our patients were cured without any relapse when using R included regimens.
Various types of central nervous system (CNS) involvement in brucellosis have been reported – e.g. meningitis, encephalitis, myelitis-radiculoneuronitis, brain abscess, epidural abscess, granuloma and demyelinating and meningovascular syndromes. 1 In our study, meningitis was determined in two neurobrucellosis cases. There are no specific guidelines regarding the antibiotic regimens and duration of treatment for neurobrucellosis. Most authorities recommend the use of D in combination with two or more other drugs, with treatment continued for several months depending on the response. 1 Drugs such as D, R and trimethoprimsulfamethoxazole have been found to be effective due to their good CNS penetration and synergistic actions. Tetracycline and STR are good for systemic brucellosis, although their CNS penetration is poor. However, as most of these patients have systemic brucellosis as well, they should, especially in initial stages, be covered with these antibiotics.1,20 Two patients in our series were treated with STR + D + R. One of these cases, a 75-year-old patient with diabetes and chronic obstructive pulmonary disease, died due to cardiopulmonary arrest at third week of treatment. Complete recovery was achieved in the remaining patient after nine months of treatment.
Combinations including STR are reported to be more effective in brucellosis cases with osteoarticular complications, particularly spondylitis. 1 There is no consensus on the duration of treatment. Although the suggested duration of treatment varies between 6 and 12 weeks, some investigators recommend continuation of treatment until the ESR returns to normal and radiological recovery is achieved.1,21 In our study, the STR + D + R regimen was administered for six weeks in all patients with osteoarticular complications. The ESR returned to normal and radiological recovery was achieved in all patients after treatment. Considering that no relapse was observed in any of the 10 patients followed-up for 18 months, triple combinations including STR may be beneficial in patients with osteoarticular complications.
There is no standard therapy protocol in chronic brucellosis. Although quinolones, STR, R, D and other antibiotic combinations and levamisole with antibiotherapy were tested for various durations, an exact treatment protocol was not recommended.1,13,22 We found that three chronic brucellosis cases were treated with two different treatment regimens. Both patients responded to treatment after three months. However, follow-up of these patients for relapse was not possible. Quinolones are recommended to be included in the triple regimen in the treatment of unresponsive chronic brucellosis. 16 But in the literature, there is no use of ceftriaxone (CAX) in chronic brucellosis, except pregnant women. 23 However, it is a reported that brucella bacteria are sensitive to CAX in vitro. 24 Also CAX added combination therapy was successful. But controlled studies, containing sufficient numbers of patients, are needed for evaluation of the effectiveness of this therapy on chronic brucellosis.
Three of the acute brucellosis cases were pregnant, in our study. Drugs, recommended in brucellosis treatment for pregnant woman are R, CAX and trimethoprim/sulfamethoxasol for between 2 and 6 weeks.23,25 In our study, pregnant women were administered CAX and R combination. Considering that three patients responded to treatment with CAX + R and that no relapse was detected in two of these during the 18-month follow-up, this combination may be successful in pregnant brucellosis patients.
In conclusion, brucellosis is a systemic infectious disease with various clinical pictures and complications. In addition to isolation and serological tests, non-specific tests such as CRP and ESR should also be used in the diagnosis and follow-up. There is no recommended treatment protocol for complicated brucellosis. Large multi-centre studies are needed to determine the most appropriate treatment choices and durations in complicated brucellosis.