
Abstract
Although postconflict Afghanistan has some of the worst health indicators in the world, the government is working hard to rebuild the health infrastructure, extend services to underserved areas and improve the quality of health services. An outbreak of cholera El Tor O1 that struck Kabul and spread nationwide in 2005, prompted a collaborative response from the Afghan Ministry of Public Health, partner agencies, and the system established to provide the Basic Package of Health Services, of which diarrhoeal disease control is an essential component. This response illustrates that, with good preparation, it is possible to respond to an outbreak of cholera effectively. The very low mortality rate during the outbreak (0.1%) shows how a resource-poor country can succeed in providing high-quality health services with government commitment, coordinated action by partners, proper case management and treatment and expanded access to services.
Introduction
The international response to Afghanistan's postconflict reconstruction and the country's steps toward a democratic and functioning government have made it the focus of world attention. The health situation in Afghanistan is one of the world's worst, and years of conflict and neglect have resulted in some of the lowest human development indicators in the world.
The maternal mortality rate is 1600 per 100,000, which translates into a lifetime chance of one in seven women dying of childbirth-related conditions. 1 The under-five mortality rate is 257 per 1000 live births. 2 Life expectancy at birth is very low (44.5 years) and Afghanistan is the only country in the world where men outlive women. 3 Literacy rates are also very low – only 29% of Afghans can read or write – and gender disparities in literacy are great: only 8% of women and 36% of men in rural areas are literate. 4 The health infrastructure has likewise been affected. A recent assessment showed that 35% of health facilities were severely damaged due to war or neglect, and the rest failed to meet World Health Organization (WHO) standards. 5
Kabul, a focus of much of the fighting, is a city with over 4.5 million residents, many of them recently returned refugees from other countries, internally displaced refugees and rural destitute populations seeking work. Kabul has no functioning public water treatment plants, water filtration systems or sewage treatment plants. A United Nations Children's Fund (UNICEF) survey 4 showed a 30% prevalence of diarrhoea among children under the age of five years in Afghanistan. Among the six major urban areas covered by the survey, Kabul city had the highest diarrhoeal prevalence rates (34%). Only 40% of the Afghan population has access to safe drinking water (urban 61 and rural 31%). 5 Communicable diseases are widespread in Afghanistan; diarrhoeal diseases are transmitted by human faecal contamination of soil, food and water.
Waste disposal systems are either poorly maintained or nonexistent, with sewage and refuse often discarded directly onto streets or in rivers and streams; awareness of and capability for safe disposal of solid waste is poor, as is awareness of personal hygiene practices. Sanitation is also poor in many households. Many people bathe in water in which waste has been disposed. Up to 53% of Kabul residents drill wells for their water supply, resulting in many households sharing water from the same groundwater table, which in Kabul is at a depth of about 10 m. 5 Pit latrines are frequently dug close to wells thus increasing the risk of spread of waterborne disease.
The winter of 2005 was severe and prolonged, with the heaviest snow pack recorded in the Hindu Kush in decades. The resultant spring runoff was unusually heavy, and floods were common in Kabul and around the country. The result was that sewage mixed with the spring water runoff and easily contaminated the water tables of Kabul and the countryside.
Recent outbreaks of cholera
Cholera has been recognized as a major public health problem in developing countries, and a significant cause of mortality, especially among children and the elderly. In an outbreak of cholera (biotype El Tor) in Peru in 1991, the initial case-fatality rate was 20%. 6 In a similar outbreak in the Congo in 1994, 20,000 deaths were recorded before the epidemic was brought under control. 7 In another outbreak in Tanzania, the case-fatality rate was 6%. 8
The El Tor Vibrio cholerae biotype has been proven to be responsible for major epidemics in Asia, Africa, the Middle East and parts of Europe since 1961. It is the biotype most often responsible for epidemics in Afghanistan. Cholera outbreaks were recorded by the WHO in 2001 in northern Afghanistan, where 114 people died. The last outbreak recorded in Kabul was in 2003, by UNICEF, with 7000 suspected cases. 9
Most cases of diarrhoea caused by cholera can be treated adequately with a solution made from oral rehydration salts (ORS). 9 During an epidemic, 80–90% of diarrhoea patients can be treated by oral rehydration alone, but patients who become severely dehydrated must be given intravenous (IV) fluids. When cholera occurs in an unprepared community, case-fatality rates may be high, usually because there are no facilities for treatment or because treatment is given too late. In contrast, a well-organized response in a country with a well-established diarrhoea disease control programme can limit the case-fatality rate to less than 1%, which is the international standard for an effective response. Poor surveillance and fear of international stigmatization and sanctions lead to underreporting of official numbers by affected countries.
Methods
Cholera outbreak in Kabul in 2005
In the middle of May 2005, reports were sent to the Ministry of Public Health (MOPH), through the newly developed health management information system, about increasing numbers of patients with acute, massive, watery diarrhoea with signs of moderate to severe dehydration. Up to 50 cases a day were reported in each of the four major hospitals in Kabul that serve as part of the sentinel surveillance system: the Infectious Disease Hospital, Indira Gandhi Child Health Institute and Maiwand Hospital – all of which are located within a few miles of each other in the centre of Kabul – and the Khair Khana Hospital – located about 10 miles north of the other hospitals. As the numbers of cases increased, officials from the MOPH began to record basic data from the patients’ hospital records, such as age, sex and address.
A pattern gradually emerged, showing that most of the early cases originated in districts 1, 2, 10 and 16, all located in the centre of ‘old Kabul’ and along the Kabul River. The poorer residents of these areas used the river for their water needs. With assistance from the WHO's Kabul office, stool samples were collected and tested by the MOPH Central Laboratory. Of the first 51 stool samples tested, 30 were confirmed as El Tor, serotype Ogawa, cholera, commonly found in Afghanistan. Because of the high rate of stools that tested positive for cholera, no further testing in Kabul was conducted. By the end of May, six deaths due to dehydration caused by diarrhoea had been reported, mostly among infants and the very old.
Officials from the MOPH responded to the outbreak by creating an Acute Gastroenteritis Taskforce chaired by the Deputy Minister of Policy and Planning to coordinate the response and assist in controlling the spread of acute watery diarrhoea. This taskforce included representatives of many partner agencies, including the WHO, UNICEF, the USAID-supported REACH (Rural Expansion of Afghanistan's Community-based Healthcare) programme, NATO, the International Committee of the Red Cross, and NGOs providing health services. The taskforce initially concentrated on supporting the affected Kabul hospitals to provide appropriate case management in order to reduce mortality. Agencies represented in the taskforce helped create separate diarrhoea treatment wards and provided tents and beds, antibiotics, IV fluids, ORS and sanitary temporary latrines.
A second major activity was an extensive behavioural change communication programme to foster improved personal hygiene and safe water practices in the community. This campaign included advice on home oral rehydration therapy and on seeking treatment at designated facilities before serious complications arise. The REACH programme had developed both print and mass media materials on diarrhoeal disease control and personal hygiene. These were rapidly distributed all over Kabul and in rural provinces throughout the country.
Table 1 shows the numbers and types of cases of dehydration from acute watery diarrhoea presenting to the four main treatment centres during July, 2005, at the peak of the epidemic.
Dehydration cases at four hospitals in Kabul
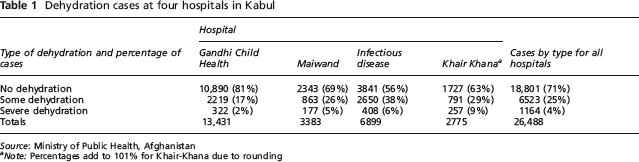
Source: Ministry of Public Health, Afghanistan
Note: Percentages add to 101% for Khair-Khana due to rounding
Over the next two months, the taskforce organized and directed the following activities in Kabul:
House-to-house hygiene education through 161,370 meetings with families in affected communities;
Periodic water samples for cholera testing;
Chlorination of 86,832 shallow wells in residential areas;
House-to-house distribution of 1,139,694 chlorine tablets and liquid chlorine in the areas most affected by the outbreak;
House-to-house distribution of 98,000 ORS packets;
Information, education and communication campaigns on personal hygiene and use of ORS for the Kabul residents most affected, including distribution of 42,000 posters, 60,000 leaflets, 400 flipcharts and 200 banners.
In addition to these activities, the MOPH, with assistance from its partners, developed a simple system for recording cases of acute watery diarrhoea, including designing and pilot-testing data collection forms, training data collectors to use them, and entering the data into a computerized database. An additional 22 sentinel surveillance sites (hospitals and clinics) for acute watery diarrhoea were identified, and information on cases was collected daily. The close monitoring of numbers of cases and deaths, and their locations in the city, assisted in the timely and appropriate deployment of supplies.
During the testing of stool samples from the provinces, the cholera serotype Inaba (which has historically been more common in Pakistan) was found, indicating that some of the cases may have travelled from Pakistan into Afghanistan. At the time, Pakistan also reported an outbreak of acute watery diarrhoea.
As the outbreak progressed, the taskforce held weekly coordination meetings and planned the transport of supplies both within Kabul and to other provinces, where confirmed cases of cholera were identified in Afghanistan's major cities and in the rural areas of many provinces. Close monitoring of the outbreak's progress made possible the prepositioning of stocks of IV fluids and ORS at the health facilities treating the largest numbers of cases. Since large supplies of IV fluids were being used by hospitals, a subcommittee of the taskforce was assigned to assess the Kabul hospitals’ consumption of medical supplies, appropriate case management of diarrhoea using ORS, and personal hygiene and disease prevention activities.
Results
This assessment showed that most hospitals had adequate supplies for managing large numbers of cases; however, hygiene standards in the wards were low and hospital personnel were overworked. The assessment also determined that health workers had good knowledge about the treatment of acute watery diarrhoea due to training that had been conducted for implementation of the Basic Package of Health Services. However, in many cases, health workers were prescribing IV fluids for patients with diarrhoea who could be treated with ORS. Table 1 shows that only 4% of patients had severe dehydration, while for the 25% with moderate dehydration, ORS could have been used more effectively.
The four major hospitals used up to 5,000 units of IV solution a day, a substantial waste of resources for patients whose records showed that ORS alone would have been adequate. The overuse of IV fluids led to shortages of IV supplies by July. Emphasis was placed on the early use of ORS when treating patients. Eventually, the supplies of IVs ran out, so ORS became the only treatment available. By August 2005, the number of new cases of acute watery diarrhoea in Kabul began to decline. Figure 1 shows the explosive rise in the number of cases of acute watery diarrhoea early in the epidemic, indicating rapid spread through the water table, and a slow decline as the summer wore on.

New cases of acute watery diarrhoea reported through surveillance systems, June–September 2005
Discussion
Overall, 62,605 people were affected by acute watery diarrhoea in Kabul during the summer of 2005. Sixty deaths were reported – a case-fatality rate of 0.1%. During the same period, 82,000 additional cases were reported from the provinces, with 110 deaths, a case-fatality rate of 0.13%. In Afghanistan, during the period 28 May to 5 September 2005, 144,605 cases of acute watery diarrhoea were reported, with 170 deaths. The overall mortality rate of 0.12% was well below the 1% commonly considered the standard for an effective response to an epidemic of cholera.
This low mortality rate can be attributed to previous preparation of the health system through the expansion of coverage of the Basic Package of Health Services in both rural and urban areas; an organized and rapid response by the MOPH and its partners; the quick activation of a surveillance system for Kabul and the provinces; prepositioning of supplies and medicines in high-risk areas; nationwide implementation of a personal hygiene and diarrhoea control communication campaign; and the previous training of Afghan health care workers in WHO diarrhoea treatment guidelines.
Strong cooperation among the MOPH and numerous partner agencies resulted in a coordinated nationwide response and effective use of available resources. It is possible for a very poor, postconflict country like Afghanistan to develop an effective response to a potentially highly fatal cholera outbreak.
Recommendations for reducing the impact of cholera outbreaks in other geographic areas based on this experience include:
Train health care workers at all levels – community, health centres and hospitals – annually in the WHO case management guidelines, before the diarrhoea season. Do not assume that all providers understand and will follow the guidelines even if they have been previously trained;
Emphasize the early use of ORS rather than IV fluids for the treatment of diarrhoea;
Carry out behaviour change communication on the importance of hygiene and hand-washing and continue communication throughout the year. In the winter, messages traditionally focus on acute respiratory infections, so the hygiene messages need to be interwoven with other health messages;
Preposition stocks of ORS and IV fluids in areas likely to experience epidemics of acute watery diarrhoea for rapid mobilization. Since large outbreaks frequently occur after flooding, prepositioning supplies minimizes transportation difficulties;
Establish a mechanism of information sharing about outbreaks between neighbouring countries, and work together to reduce the ‘stigma of quarantine’ that inhibits accurate reporting about outbreaks;
Promote the use of chlorine products for food and water purification at the point of consumption, and distribute them to the population at the beginning of the hot season;
Promote safe disposal of solid wastes (in latrines), and educate the population about how to site them away from water sources;
Develop an early warning system for the detection and confirmation of cholera cases that will lead to the rapid initiation of a response plan. This surveillance system will require regular maintenance;
Involve all donors and partners in nationwide planning before an epidemic. Define the role of every organization clearly and make sure each has committed the resources needed to implement the plan.
Footnotes
Acknowledgements
Funding for this article was provided by the United States Agency for International Development under the REACH programme, contract number EEE-C-00-03-00021-00. The opinions expressed herein are those of the authors and do not necessarily reflect the views of USAID.