
Abstract
Angola currently has the second mortality rate for children in the world. A cross-sectional study was performed containing 1322 random selected children of the 10288 hospitalized from December 2004 to May 2005 at the Hospital Pediátrico David Bernardino, the largest hospital in Angola and health reference centre located in the capital city of Luanda. Hospital mortality was 18% and the main causes of death were:malaria (22.4%), undernutrition (21.5%), pneumonia (11.8%), neonatal affections (9.3%) and meningitis (8.0%). Programmes must be rapidly implemented to eradicate undernutrition, improve perinatal care and control infections, especially malaria, pneumonia and meningitis.
Child mortality in sub-Saharan Africa is 29 times higher than in industrialized countries. Located in sub-Saharan Africa, Angola, with an estimated population of 13 million inhabitants and a life expectancy of 39.9 years, currently has a mortality rate of 260/thousand for children under 5 years of age: the second highest mortality rate in the world, only exceeded by Sierra Leone.1,2
In developing countries health information systems face serious difficulties. In Angola, this situation was particularly aggravated by the civil war following the country's independence in 1975, which lasted until 2002. During that time basic services in health and education were severely affected. Information on hospital morbidity and mortality, that could offer important inputs for public health policies planning, is still unavailable in Angola. 3
The Paediatric Hospital David Bernardino (HPDB), a health reference centre located in the capital city of Luanda, is the largest hospital in Angola. It has 296 beds and caters for about 27,000 hospitalized children per year. 4
The aim of this study was to determine the causes of death of children hospitalized in Luanda. A cross-sectional study was performed containing 1322 of the 10,288 patients admitted from December 2004 to May 2005. This sample was collected at random from a list of numbers obtained via the Epitable module of EPIINFO 6.0.
All data were collected during hospital admission and at discharge by one of the researchers (EAP). The study was approved by the Ethics Committee of the HPDB and the guardians of the children studied signed an informed consent form.
Of the 1322 children admitted, 237 (18%) died. Their ages varied from 0 to 11 years old (x = 11.3 months; standard deviation [SD] = 5.3) – of these 144 (61%) were boys. Some degree of undernourishment was found in 189 (80.7%), which was severe in 91 (38.4%), according to the weight-for-age World Health Organization (WHO) criteria (Table 1). 5
Causes of death and the nutritional status of hospitalized children in Luanda, Angola, 2005
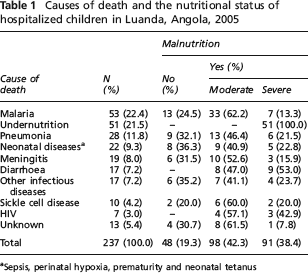
Sepsis, perinatal hypoxia, prematurity and neonatal tetanus
The mothers’ ages ranged from between 15 to 47 years old (x = 26.2 years; SD = 3.7); 95 (40.1%) were illiterate and 39 (16.4%) had less than four years schooling. Two hundred mothers (84.3%) were multiparous, and 113 (47.6%) had already lost at least one child. Seventy-seven (32.5%) were unemployed.
The main causes of death are shown in Table 1.
In Angola, only 5% of about 16.900/year children under five deaths take place at the hospitals. Although we have analysed only the in-hospital mortality we believe that these data focus the interaction of nutrition and infectious illnesses in Angola.
Mortality rates from malaria and pneumonia were similar to other countries in sub-Sahara Africa. 2 The hospital malnutrition case fatality was far above the WHO expectation of 5%. In some African countries the case fatality rate is >50% with the risk of mortality being five to eight times greater among severely malnourished children. 6 The implement of the WHO protocol for the hospital management of severely malnourished children has been shown to reduce hospital mortality caused by severe malnutrition. 7
The main causes of neonatal mortality were: sepsis, perinatal hypoxia, prematurity and neonatal tetanus. Neonatal mortality accounts for 47% of the total mortality in under 5–year-olds in developing countries; our results (9.3%) show a high post-neonatal mortality. The low diarrhoea mortality could be explained by the presence of an oral hydratation unit at the HPDB. Other infectious diseases were almost all soft tissue infections. Death rates caused by the sickle cell disease were similar to those seen in other African countries. The massive population movement that occurred at the end of the civil war has been of great concern in Angola. However, the HIV levels detected to date are low in comparison with other sub-Saharan countries.
We believe that these data should be taken into consideration when designing strategies to reduce mortality in hospitalized children in Luanda, Angola. It is therefore imperative that programmes are rapidly implemented that are designed to eradicate undernutrition, improve perinatal care and control infections (especially malaria, pneumonia and meningitis).