
Abstract
We undertook this retrospective cross-sectional study in order to establish the outcome of 510 singleton breech presentations at term in seven district hospitals in rural Matabeleland-North Province, Zimbabwe. We also studied the mortality for 1093 caesarean sections (CS), in order to decide if CS should be the preferred option for breech births.
The perinatal mortality rate in singleton breech presentation (BrPNMR) was very high:166/1000. Between the hospitals the BrPNMR ranged from 66 to 225/1000 (P = 0.04). Although the outcome was better for CS than for vaginal delivery (odds ratio = 5.4, P = 0.0005), there was no correlation between the BrPNMR and the CS rate. Results indicate that closer monitoring of these high-risk pregnancies by the most senior staff would be more effective than increasing the number of CS performed. An external cephalic version at term could also reduce breech-related mortality.
Symphysiotomy is a life-saving emergency intervention when the head is trapped. Increasing the number of CS should be strongly discouraged since the case fatality rate in this rural setting was found to be very high: 18/1093 women died after CS (for any indication) within 42 days after the operation (1, 6%); 15 within 24 h. Haemorrhage was the major cause of death.
Introduction
The management of breech presentation has been a controversial issue for many years. In 2000, the first large multicentre randomized trial (the Term Breech Trial) by Hannah et al. showed that planned caesarean sections (CS) resulted in significantly lower perinatal mortality and morbidity compared to vaginal delivery. 1 However, the setting of Hannah's study of central hospitals, with experienced gynaecologists and planned deliveries, does not reflect the reality of the average district hospital in a low-income country. Few data are available on the outcome of breech presentations (BrPNMR) in sub-Saharan Africa and most studies were done in a central hospital context.2–7
A retrospective cross-sectional study was conducted in the district hospitals of rural Matabeleland-North Province to consider the appropriateness of CS as the preferred mode of delivery for breech presentations. We compared the outcome of singleton BrPNMR at term after CS and vaginal delivery (1996–2001) and then established the mortality rate related to CS in the province (1998–2000).
Methods
Matabeleland-North Province is situated in the western part of Zimbabwe. Its population of about 815,000 (in 1999) – 85% rural – is distributed over seven districts. Seven (acting) district hospitals were included in the study: five public hospitals and two missions (one hospital became operative in 1999). A large private mine hospital was excluded, as well as a small mission hospital where no CS were performed. Five of the seven hospitals had at least one resident medical officer for most of the time, usually a young general doctor with a few years experience. There were no gynaecologists at district level. If during antenatal care a midwife in one of the rural clinics detected a possible breech presentation after 36 weeks, she would refer the woman to the nearest hospital for delivery. All hospitals had beds or shelters for waiting mothers.
Singleton breech presentations
Delivery at term was defined as a birth weight of 2500 g or more. All singleton breech deliveries of 2500 g or more between 1 July 1996 and 30 June 2001 were included. Information was extracted from the maternity registers on age, parity, bad obstetric history (defined as history of perinatal death or CS), person who assisted the delivery, type of delivery, birth weight and outcome. Where available, the patients’ notes were used to confirm the data from the maternity registers. Few discrepancies were found. Some data were missing altogether. From the patients’ notes, we also collected information on dilatation on admission in the maternity ward, progress of dilatation, assessment by a doctor during the first stage of labour and use of the partogram. Deaths after discharge (for vaginal deliveries after 24 h and for CS after one week) were not included. Breech-related perinatal mortality (BrPNM) refers to the stillbirths and early (first week) neonatal deaths among the hospital breech deliveries only.
Deaths after CS
A death after CS was defined as any death of a woman during, or within 42 days after, an abdominal operation to deliver a baby (for any indication) including surgery for rupture of the uterus. We scrutinized delivery registers, admission books, hospital medical records, maternal mortality notification forms and monthly mortality reporting forms for the three-year period 1998–2000. The following information was recorded on a checklist: numbers and place of deliveries, numbers of CS and their indications; number, causes and circumstances of deaths.
Data analysis
For data entry and analysis, we used EPI INFO 6 software and Stata version 7.0. We performed logistic regression to compare the outcome of breech presentation after vaginal delivery and CS.
Results
Perinatal mortality in term breech presentations
A total of 33,710 babies were reportedly born in the seven district hospitals during the five-year period of study, about a quarter of all deliveries in the province, of which 510 were singleton breech weighing 2500 g or more (1.5%). The characteristics of these deliveries are summarized in Table 1. Of the mothers 11.6% had a bad obstetric history, including one or more previous CS (8.6% of all deliveries). The BrPNMR was 166/1000 (95% confidence interval: 133–199). The macerated stillbirth rate was 22/1000 and the fresh stillbirth rate 81/1000. Early neonatal mortality rate was 70/1000 live births. 75/1000 live births were a live on discharge but had an Apgar score below 7 after 5 minutes. Seventeen babies (34/1000) had congenital abnormalities of whom only five survived. In total, 123 out of 510 births (241/1000) had a poor outcome, i.e. perinatal death, Apgar score below 7, or severe congenital abnormality.
Characteristics of all term breech deliveries (n = 510) seven district hospitals in Matabeleland-North, 1996–2001
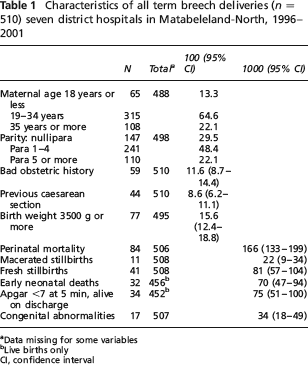
Data missing for some variables
Live births only
CI, confidence interval
In a further analysis we compared the outcome of vaginal delivery versus CS in the BrPNMR. We excluded all cases from hospitals which did not have a resident medical officer for most of the time. Also excluded were all cases in which the choice between vaginal delivery and CS was clear-cut: intra-uterine deaths (16), placenta praevia (1), severe neural tube defects (12) and other congenital abnormalities (2). For the remaining 359 cases the BrPNMR after CS was 38/1000 vs. 175/1000 after vaginal delivery (crude odds ratio [OR] = 5.4, P = 0.0005). The difference was mainly due to a higher fresh stillbirth rate at vaginal delivery (P = 0.0006; there was no OR as there were no fresh stillbirths after CS). The early neonatal mortality rate was similar in both groups (P = 0.24). The percentage of babies alive on discharge after an Apgar score below 7 after 5 min did not differ either (P = 0.23). Adjustment for age, parity, bad obstetric history, dilatation at arrival, assessment by doctor during first stage, birth weight and hospital did not change the results.
Marked differences were found in management and outcome of breech deliveries between the different hospitals in the province (Table 2). Differences in management appeared in the use of the partogram (range: 46.0–81.4%; P = 0.002), the percentage of vaginal deliveries done by a doctor (range: 14.8–56.2%, P < 0.001) and the CS rate (range: 22.8–52.4%; P = 0.003). Some hospitals had a far better outcome than others, with the BrPNMR varying from 66 to 225/1000 (P = 0.04). There was no correlation between the BrPNMR and the CS rate per hospital (chi square for trend = 0.01, P = 0.97). Indeed, although hospitals 2 and 3 had a high CS rate they had an average BrPNMR and hospital 5 which had an average CS rate had the lowest BrPNMR.
Differences in management and outcome of breech deliveries (n = 359 a ) in five selected district hospitals with a generally present medical officer in Matabeleland-North, 1996–2001
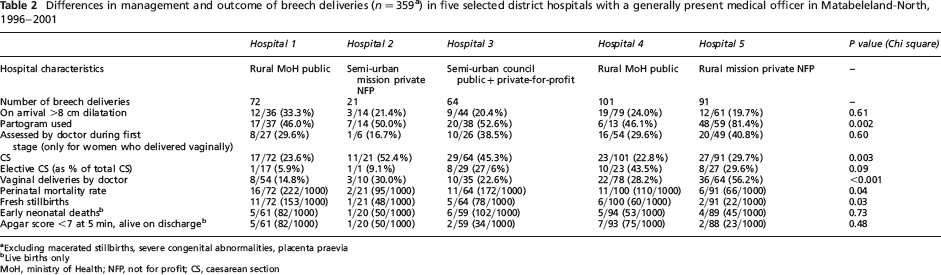
Excluding macerated stillbirths, severe congenital abnormalities, placenta praevia
Live births only
MoH, ministry of Health; NFP, not for profit; CS, caesarean section
Mortality after CS
Of the 21,902 deliveries reported in the three-year period 1998–2000, 1128 ended in a CS (5.2%, range between hospitals = 2.1%–9.8%) complicated by 18 deaths (1.6%, ranging from 0.5% to 3.8% between hospitals). Haemorrhage ranked highest as a direct cause of death (10/18; five were women with a previous CS), followed by anaesthetic accidents (three, of whom one woman had a previous CS) and sepsis.
Discussion
The most striking finding of this study is the high BrPNMR of 166/1000 term breech presentations. This is probably an underestimation, as not all early neonatal deaths after discharge were captured. Studies in sub-Saharan Africa report a BrPNMR between 62 and 156/1000 in central hospitals that had a gynaecologist.2–6 Our results compare favourably with the 332/1000 found in a sample of 44 breeches in a similar setting in Zambia. 7 During the period of study the perinatal mortality rate for all institutional births in this province was 64/1000. 8
Though birth by CS had a better outcome than vaginal birth, a comparison between hospitals shows no correlation between the BrPNMR and the CS rate. Hospital 5 with the lowest BrPNMR has a relatively low CS rate. It is a mission hospital, marked by regular use of the partogram and frequent presence of a medical officer during first and second stage of labour. Hospital 1 is a government-run hospital with the poorest outcome and a low CS rate. The poor outcome can be explained by other factors: this hospital is situated in the least developed area of the province; women present late, sometimes in advanced labour; only a minority of the women is assessed and/or delivered by the doctor.
Our second finding of a very high case fatality rate of 1.6% related to CS (for any indication), is a reason for great concern. We calculate that delivering 1000 babies in breech presentation by CS (excluding those whose outcome cannot be influenced by labour management) would save 137 babies, while 16 mothers would die as a result of the operation. Assuming that each woman will have two more deliveries and one third of these will be by CS, this policy would cause 656 (984 2/3) additional CS in the future, and 11 more maternal deaths, and this does not include the women who will die from a ruptured uterus during a subsequent pregnancy before they can have a repeat CS. Therefore, delivering all term breech presentations by CS would save 137 babies, but at least 27 women would die. In our view this is totally unacceptable. In addition, orphaned babies also have a high risk of dying.
In this rural setting only a minority of women deliver in district hospitals. Thus, women with an easy vaginal breech delivery (at home or in a clinic) resulting in a live baby were not taken into account in this study. If all breech presentations at term were delivered by CS, then even more CS would be performed but a lower percentage of babies would benefit.
The lack of correlation between the BrPNMR and the CS rate, and the high mortality rate after CS, make a strong case against the systematic delivery of BrPNMR by CS in this setting. Rather, attention should be given to improving the overall management of breech deliveries:
Recognition of breech presentation at antenatal clinics; Early admission to a waiting mothers’ shelter; Good management of labour with use of a partogram; Assessment and delivery by the most senior person in the hospital.
Use of external cephalic version (ECV) at 37 weeks, a proven safe and effective technique in experienced hands, could considerably improve the outcome.9,10 Doctors should also always be prepared for an emergency symphysiotomy – a life saving intervention, when the head is unexpectedly trapped.11,12
That this approach can be successful is supported by the experience in hospital 4, where the policy was changed after a discussion of the results of the above study. The hospital's new policy determines that each woman with a breech presentation should be seen by a doctor at 37 weeks for pelvic assessment and ECV and that she should be given an ultrasound to exclude any gross abnormalities and to estimate the birth weight. Each woman with a breech presentation in labour should be assessed by the doctor and the doctor should be present at delivery. In 2002, the year after the policy change, only one out of 20 babies with breech presentation died (a fresh stillbirth in a woman with three previous stillbirths who arrived fully dilated) and none of the surviving babies had an Apgar score below 7 after 5 min. Of the vaginal breech deliveries 71% were done by the doctor. The CS rate in breech presentations rose slightly from 22.8 to 30%. However, no ECV was performed, due to a lack of confidence on the part of the staff and the difficulty of organizing an assessment at 37 weeks.
Conclusions
The outcome of singleton breech presentations at term in rural Matabeleland-North Province is very poor. The results indicate that improved monitoring of breech presentations by the most senior staff during labour and delivery will have a positive impact on the outcome.
Because of a lack of correlation between the breech presentations and the CS rate, and a very high case fatality rate after CS of 1.6%, systematic delivery of BrPNMR by CS in this rural setting is strongly discouraged.
Waiting mother shelters should be available at all hospitals for women with at-risk pregnancies. ECV at term could, in theory, also have an important impact on the outcome – but at the moment medical the staff in these district hospitals lacks the expertise to apply this technique. Symphysiotomy can be a life saving intervention and all doctors should know how to carry it out.
Footnotes
Acknowledgements
The authors would like to thank Mr A Nyanhete, Tsholotsho District Health Executive member, as well as the Health Information Clerks of Binga, Bubi, Hwange, Lupane, Nkayi, Tsholotsho and Umguza districts for their assistance with the collection of data.