
Abstract
The basic component of the new World Health Organization (WHO) antenatal care model prescribes reduced number of clinic visits and limited investigations for low-risk pregnant women. The objectives of this study were to determine the proportion of pregnant women seeking antenatal care in a Nigerian teaching hospital who qualify for the basic component and to document difficulties that may arise with the classifying form.
In December 2004, 234 pregnant women who had initiated antenatal care were enrolled for the study. Using the classifying form, 157 (67%) were eligible for the basic component, 41 (18%) for special care, but 36 (15%) women could not be classified. Those that did not know the birth weight of their last babies accounted for most (89%) of the unclassified group.
The WHO antenatal care model was the most appropriate and relevant method for our hospital where a large percentage (67%) of prenatal women were eligible for the basic component. However, we consider that the classifying form should be adapted to accommodate all pregnant women.
Introduction
Antenatal care has been practiced in much the same way in most countries for the past 55 years. To a large extent, developing countries have adopted the antenatal programmes of developed countries with only minor adjustments in terms of endemic disease. 1 In the standard model of antenatal care, low-risk pregnant women are seen monthly until week 28, then fortnightly to week 36 and weekly until delivery. The results of the World Health Organization (WHO) antenatal care randomized trial, 2 and the systematic review of the scientific evidence on models of antenatal care utilizing a reduced number of visits, justified the introduction of a new WHO model for general use. Such a model is even more relevant for developing countries where staff and resources are scarce.
In some low-resource countries, the stratification of health services into primary, secondary and tertiary levels is mainly academic as patients criss-cross the various levels in no particular order. For example, in urban areas patients who should attend a primary health clinic or a secondary health facility would often go directly to the teaching hospital without a referral and would not be denied care. This tends to put pressure and strain on some health facilities whilst others are under utilized or used less efficiently.4,5
At the Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto, Nigeria, services are highly subsidized and, therefore, widely used putting enormous pressure on the infrastructure. In the maternity unit, the old standard model of antenatal care is still used. The need for change became obvious after the publication of the results a randomized-controlled trial 2 that compared the standard model with a new WHO model which limits the number of visits and restricts investigations to those that have been shown to improve outcomes for women and newborns. However, such a change must be gradual and, in our setting, the new model may have limitations.6,7 The objectives of this study were to determine the percentage of pregnant women that would benefit from the basic component of the WHO model in a teaching hospital setting and to document difficulties that may arise using the classifying form in its present form.
Materials and methods
Pregnant women who initiated antenatal care in December 2004, at the maternity unit of the UDUTH were enrolled for the study after appropriate counselling. The WHO classifying form (Figure 1) was used to decide which women qualify for the basic component of the new model and which will require special care. Women that answered ‘no’ to all of the 18 questions on the classifying form were eligible for the basic component (reduced visits, limited investigations); a ‘yes’ to any of the questions meant special care. The third category was for women who could not be classified because they could not answer ‘yes’ ‘or’ no’ to some of the questions.
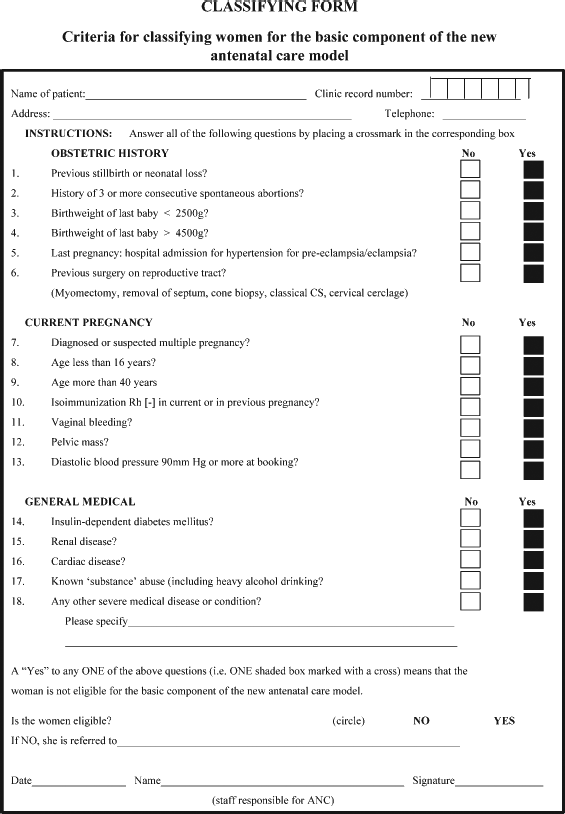
World Health Organization classifying form
Results
Two hundred and thirty-four pregnant women were recruited into the study using the new WHO model. The distribution of the women into the various groups is shown in Table 1. Thirty-two women in the unclassified group did not know the birth weight of their previous babies because that had opted for home confinement. Three women had caesarean section elsewhere but we were unable to ascertain which method had been used. Among the unclassified group, one woman had two previous lower segment caesarean sections.
Distribution of pregnant women using the World Health Organization classifying form

Discussion
The new WHO antenatal care model separates pregnant women into two groups, namely, those eligible for a schedule of four visits and those who need special care based on their specific health conditions. The basic component of the model is intended only for the management of pregnant women who do not have evidence of medical or pregnancy-related complications: hence, the number of clinic visits is reduced and investigations restricted to only those that have been shown to have an improved feto-maternal outcome. Of the pregnant women in our study 67% were eligible for the basic component of the model. This is not as high as the 75% predicted by WHO, 8 but it is a large percentage considering the fact that the facility is a teaching hospital meant primarily for high-risk patients. It is also possible that the percentage would have been higher if we had been able to classify all women correctly. We postulate that the higher the proportion of pregnant women who are eligible to receive the reduced visit schedule, the more relevant the new WHO model is to a health facility.
A reduced number of visits and investigations associated with the basic component should mean more time for providers to attend to women requiring special care and for other activities. Evidence already exists showing the effectiveness of this new model.9–12 However, an assessment of patient and provider satisfaction is also needed.
The best way to manage those women who could not be classified using the present classifying form has yet to be determined. Some women will not know the birth weight of their babies because of home delivery and/or the non-availability of a skilled birth attendant. We propose that if a baby who has been delivered at home is still alive and well it should be possible to enter the mother into the reduced schedule visit model even if birth weight is unknown. Only a few could not be classified due their being unsure of the type of caesarean section they had received. Such women should be entered under the special care category and managed accordingly.
In conclusion, a large percentage (67%) of pregnant women seeking antenatal care in our teaching hospital qualified for the basic component of the WHO antenatal care model. Therefore, the use of the model is appropriate and relevant in our setting, enabling resources and time to given to other activities. However, the classifying form needs to be modified so that we can categorize all the pregnant women in our setting.