
Abstract
SUMMARY
Tea preparations from the herb Artemisia annua L. (Aa) which is used in traditional Chinese medicine might offer an inexpensive way of producing artemisinin drugs locally. We compared Aa with sulfadoxine-pyrimethamine (SP) in the treatment of uncomplicated falciparum malaria in semi-immune adults. After seven days, the cure rate was 7/10 for the Aa compared to 7/9 for SP; this dropped to 4/10 for Aa and 4/9 for SP at day 14 and to 1/9 for Aa and 3/8 for SP at day 28.
Introduction
Malaria, the most important parasitic infection causes more than a million deaths annually. 1 This disease hits households in poor communities the hardest, despite the existence of effective anti-malarial tools and interventions. Artemisinin-based anti-malarial therapy is effective, 2 but expensive. The herb Artemisia annua L. (Aa; annual wormwood) has been used in traditional Chinese medicine for the treatment of febrile diseases and malaria for many centuries. Its cultivation is relatively easy. 3 Tea preparations from Aa, prepared according to the current pharmacopoeia of the People's Republic of China, resulted in peak plasma levels of 240 ng/mL artemisinin in humans. 4 There have been several open-labelled clinical trials, 3,5 but we decided to conduct a randomized double-blind clinical trial evaluating the efficacy and safety of Aa tea preparations in the treatment of Plasmodium falciparum malaria.
Methods
The study was performed in a rural hospital in the Kigoma region of western Tanzania from September 2002 to March 2003. The protocol was approved by the ethical committee of the National Institute for Medical Research, Dar-es-Salaam, Tanzania. All patients gave written informed consent. Inclusion criteria were: P. falciparum malaria with parasitaemia between 2.000/µL and 40.000/µL; a minimum age of 18 years; residence in rural Kigoma or the Kasulu district for ≥5 years; and at least one of the following clinical symptoms – fever, chills, fatigue, vertigo, nausea, joint pain, vomiting, headache or abdominal pain. The exclusion criteria included: pregnancy or lactation; treatment for malaria within two weeks before recruitment; any clinical signs of complicated malaria; current medical treatment (modern or traditional) for other diseases; and known chronic, progressive or life-threatening diseases. Before randomization, and after seven days of medication, urine samples were examined by thin layer chromatography for medication with other anti-malarial drugs, and positive patients were excluded.
Patients were randomly assigned to one of the following treatment groups: A5 and A9 groups: Aa tea (5.0 g and 9.0 g herb/L, respectively); 1 L/day for seven days and placebo tablets day 1. Sulfadoxine-pyrimethamine (SP) group: sulfadoxine 25 mg/kg and pyrimethamine 1.25 mg/kg day 1 and placebo tea Radix Gentianae 3.5 g/L, 1 L/day for seven days.
The zero hypotheses were that at day 7 there would be no difference in the cure rate between the three groups. A difference would be defined as proportions showing a difference of 20% or more. The equivalence should be tested on a 5% significance level with 90% power. We presumed a cure rate at day 7 of CRSP 90% in the SP group and a cure rate of CRHAa 90% for the groups treated with the Aa-tea preparation. To meet the criteria, at least 48 patients per group who fitted the protocol would be needed; we planned to enrol 60 patients per group. Randomization was done by opening opaque envelopes prepared in blocks of 30 patients.
The Artemisia annua L. cv. Artemis (artemisinin content 1.4%) was supplied by Anamed, Waiblingen, Germany, and pre-packed in sealed plastic bags in doses of 5 and 9 g. The tea was prepared freshly in accordance with method C described by Rath et al. 4 Radix Gentianae was supplied by Caesar & Loretz, Hilden, Germany, and prepared in the same way. The tea preparations looked and tasted the same. SP was supplied by Pharmamed, La Valletta, Malta (Ch:16800071B).
Pulse, blood pressure and body temperature were recorded daily until day 7. On days 3, 7, 14 and 28 patients were interviewed using a standardized questionnaire for clinical symptoms and adverse events. Parasitaemia was determined from a finger prick using Field-stained thick blood smears. The number of trophozoites was counted in 100 high power fields.
The primary endpoint was the parasitological cure rate, i.e. the proportion of patients with negative blood smears on day 7. Secondary endpoints were cure rates on days 14 and 28, and a change of clinical symptoms. Criteria for treatment failure were: the development of severe malaria or danger signs; parasitaemia on day 3 equal or higher than the parasite count on day 0; parasitaemia on day 7 and any recurrence up to day 28. Treatment failures were appropriately treated.
Results
After randomization, we had to exclude four patients for the reasons shown in Figure 1. The baseline characteristics of the patients included in the analysis are shown in Table 1. The high rate of recrudescence in all patients randomized and treated according to protocol led to the decision to end patient recruitment in March 2003. Most of the reported malaria symptoms improved or resolved within three days after initiation of therapy – as quickly in the SP group as in the Aa groups (data not shown). We observed two adverse events not distinguishable from malaria-related symptoms. Due to excessive vomiting, one patient in the SP group had to be treated with quinine from day 2. One patient in the Aa 9 g/L group developed hyperparasitaemia and clinical signs of cerebral involvement at day 1 and was switched to quinine treatment. The Aa preparations were well tolerated.
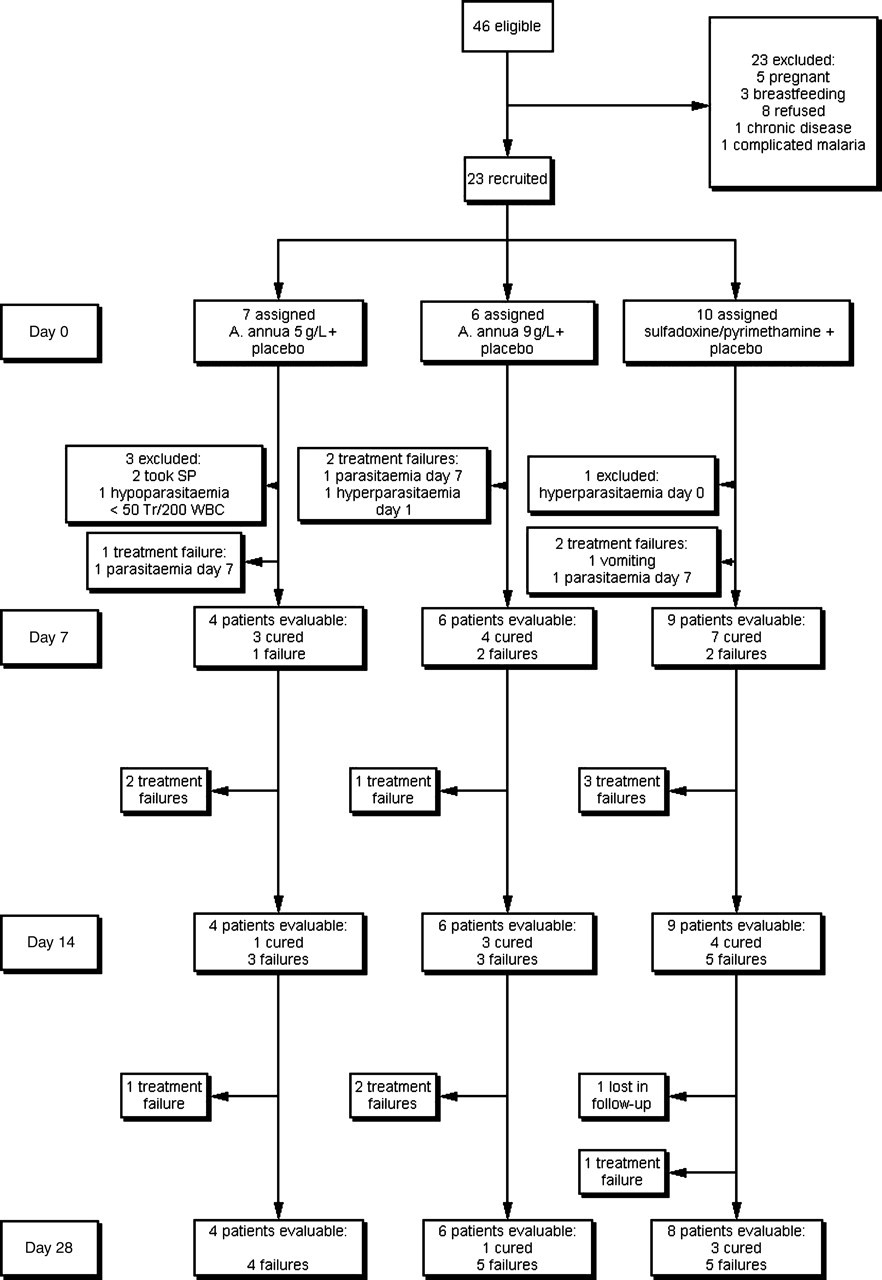
Trial profile
Baseline characteristics of the patients
Discussion
Despite the small number of patients recruited, our primary cure rates in the Aa groups at day 7 were similar to the 74% reported my Müller et al. 5 in their open pilot trial. Follow-up of patients was almost complete and showed high rates of recrudescence. Artemisinin-based combination therapy is being introduced in the treatment guidelines of several countries in sub-Saharan Africa. The expensive part is the artemisinin derivative. Local cultivation of Aa and the preparation of medicinal tea would reduce costs and might therefore be a consideration for financially restricted health systems. However, the artemisinin content of the traditional Aa preparations contained, at best, 94 mg artemisinin/L, 4 i.e. 19% of the usual clinical dose of pure artemisinin (500 mg/day). Insufficient doses and incomplete treatments without complete cure are major reasons for the induction of resistance to many antimalarials. Inappropriate drug use in artemisinin-based combination therapies in French Guiana exerted selection pressures that favoured led to the emergence of parasites with an artemether-resistant in-vitro profile. 6 Therefore, it is important to introduce a risk assessment of the use of Aa tea preparations in treatment schedules in order to avoid under-dosing and to ensure patient compliance.
We conclude that mono-therapy with a tea preparation of Aa cannot be recommended for the treatment of uncomplicated falciparum malaria in adults.
Footnotes
Acknowledgments
We are grateful to all study participants. We thank E J Kebelo for his help in the laboratory work, A Jäger MD in the clinical follow-up and H Bönning in the enrolment of patients, allocation to treatment groups and application of drugs. We also thank Mrs Gründler, Paul-Lechler Hospital Tübingen and DR J W Bailey, Liverpool School of Tropical Medicine and Hygiene for the quality control of thick films and M Tabende, Bukavu D R, Congo for training in thin film chromatography. We were sponsored by the German Institute for Medical Mission, Tübingen and Christliche Fachkräfte International, Stuttgart, Germany