
Abstract
SUMMARY
Although much general information has accumulated about ocular myiasis, there are very few reports about the same amongst the Indian population. We present a case series, comprising of 13 documented cases of external ophthalmomyiasis due to Oestrus ovis, detected at regular intervals in a small geographical area of rural central India, which strongly indicated the presence of a previously unknown endemic eye disease of this region.
Introduction
Ocular involvement occurs in about <5% of all cases of human myiasis. 1 Ophthalmomyiasis is categorized as ophthalmomyiasis externa if the maggots are confined to the external surface of the eye and ophthalmomyiasis interna if they penetrate the ocular coats to reach the intraocular structures.
The sheep nasal botfly (Oestrus ovis; family – Oestridae), an endoparasite in the nasal cavity of sheep and goats, is the most common causative agent of external ophthalmomyiasis. 2 Some cases have been reported from some Mediterranean countries as well as Iraq, North America, Australia and South Africa. 3–6 To the best of our knowledge, only three case reports from different parts of India have so far been reported. 7–9 During our six year study of a small geographical area of rural central India, we came across 13 proven cases of ophthalmomyiasis due to larvae of O. ovis. This tempted us to consider the possibility that ophthalmomyiasis due to sheep nasal botfly might be endemic to this particular area. We therefore decided to study these cases which were given wide local publicity.
Material and methods
During a period of six years between September 2000 and September 2006, we came across more than 20 patients who gave a history of worms crawling out from their eyes. However, worms could be isolated only from 13 of them, and we faced some difficulty in identifying the causative agent with the first of this series of patients.
The first case, a 34-year-old woman patient came to our outpatient department with a two-day history of a mild foreign body sensation, redness and watering from her right eye. She also complained that small worms were crawling out of her eye. She brought one of them in a small bottle. We examined both her eyes. The right eye showed mild oedema of the eye lids along with conjunctival congestion. Rest of the anterior segment did not show any unusual findings. There was no discharge from the right eye. Visual acuity was 6/6 for distance and N6 for near. On a slit-lamp examination, a number of tiny translucent worms, 1–2 mm in size with dark heads, were found to be crawling over the bulbar conjunctiva and a few were aggregated in the lower fornix. The larvae actively avoided the bright light of the slit lamp and tried to burrow deep into the conjunctival fornices. Using a topical anaesthesia with 4% lignocaine, these larvae were removed with the help of fine forceps and mounted on a glass slide for identification. Direct and indirect ophthalmoscopy showed no evidence of internal ocular inflammation. Examination of left eye was within normal limits.
Topical steroid and antibiotic drops were prescribed. When the patient came for follow up two days later, all symptoms had been resolved to a great extent. A repeat slit-lamp examination did not reveal any more larvae and the fundus examination was normal. Slide-mounted larvae were sent for photography and, along with the microphotographs, they were sent to the department of microbiology for identification. However, our medical microbiologists were unable to identify them conclusively. The larvae were finally identified as those of O. ovis by an entomologist from the zoological survey of India. We then decided to record all such cases and give them high level publicity locally.
Results
Over a period of six years, we identified 13 cases of ophthalmomyiasis due to the larvae of the sheep nasal botfly, O. ovis. The results are shown in Table 1 in which it is clear that almost all of the patients came from rural households whose main occupation was farming and many of them reared sheep. The ages ranged from a four-year-old schoolgirl to a 56-year-old farmer. Many reported being attacked by an insect. Although, larvae could be identified from all of these patients, in none were there any signs that the interior of the eye had been involved.
Details of cases of 13 cases of external ophthalmomyiasis
M, male; F, female; +, positive; −, negative
Were these case findings of any epidemiological value? If yes, why had it not been reported before? Was a new disease in this geographical area or had it gone undetected for some time? We raised these queries at the district ophthalmologists' forum. To our surprise, most of the ophthalmologists present reported that they too had come across similar cases. Some had thought that they were house fly maggots and treated them symptomatically. Some were interested but unable to investigate further due to the non-availability of a clinical microbiologist. Most of had come across patients presenting with similar complaints. This exchange of information with neighbouring ophthalmologists further strengthened our suspicion that ophthalmomyiasis due to O. ovis was endemic in this area, especially since sheep raising was common among these farmers.
Discussion
Endemic means that there is a constant presence of a disease or infectious agent within a given geographic area or population group, without importation from outside. It may also refer to the usual or expected frequency of disease within such an area or population group. The most common cause of ophthalmomyiasis is the first-stage larvae (Figure 1) of the sheep nasal botfly (O. ovis). 1 The adults are bee-like flies whose natural hosts are sheep. O. ovis normally deposit the first-stage instar (immature) larvae in the nostrils of sheep. Some authors have claimed that human infection is more common where there are fewer sheep present in an endemic area.

A microphotograph showing a fist-stage Oestrus ovis larva (×40)
The adults hover over the target and eject a spray of larvae on to the sheep. The larvae attach themselves to the mucous membrane of the nose and penetrate the sinuses. The maggots develop into second and third instar larvae in the sinuses. When mature, the larvae fall from the nose to the ground and pupate. Adult flies emerge from pupae after three to six weeks and may live for up to a month. 1
Typically, patients complain of being struck in the eye by an insect or a foreign object. Within a few hours painful inflammation occurs, which may last for a few days as the larvae cannot develop any further in man. Occasionally, larvae reach the nasal cavities (its natural habitat in sheep and goats) where they cause swelling and pain as well as frontal headaches. However, they do not live longer than 10 days. 1 They are also equipped with oral hooks (Figure 2) and spines and can burrow into the lids or penetrate the globe through the sclera into the inner structures of the eye, causing internal ophthalmomyiasis. 1,10 The consequent panuveitis is often severe and the visual prognosis poor. Debilitated elderly people and poorly nourished children are particularly susceptible to internal ophthalmomyiasis. In very severe cases, particularly in tropical countries where the standard of hygiene is low, the maggots eat into the tissues and convert the whole orbit into a crawling pit. The treatment for external infestation (ophthalmomyiasis externa) is the surgical removal of all the larvae from the conjunctival sac followed by the administration of steroid drops to reduce inflammation and antibiotic drops to prevent or treat secondary infection. Agents such as topical lignocaine, liquid paraffin and 10% ethylether in vegetable oil can be used to anaesthetize and asphyxiate the larvae before removing them with a fine forceps. If the disease spreads to the interior of the eye (ophthalmomyiasis interna), the resulting uveitis and endophthalmitis may require aggressive treatment such as vitrectomy and intra vitreal instillation of antibiotics, where the visual prognosis remains poor.
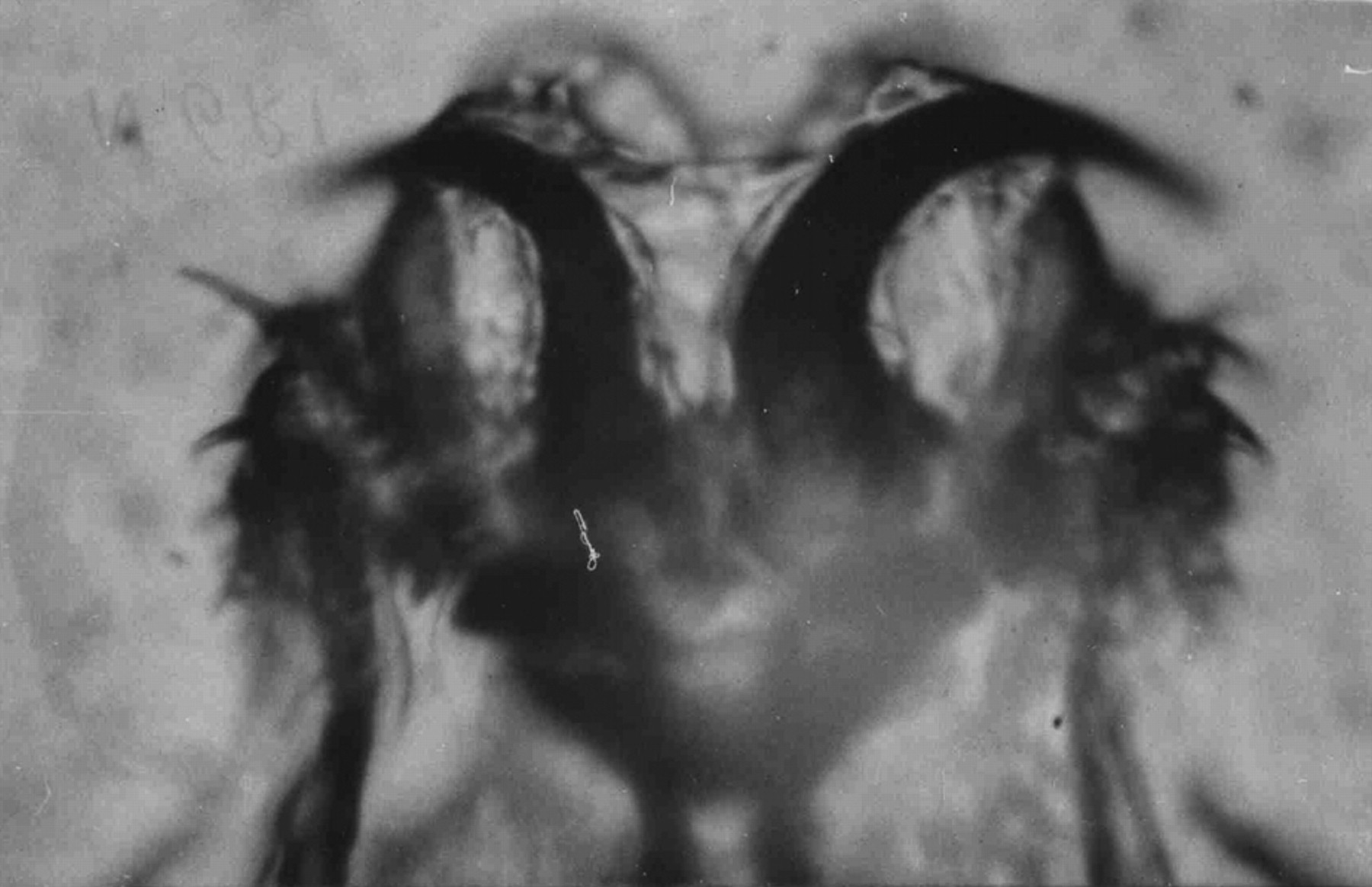
A microphotograph of the oral hooks of an Oestrus ovis larva (×40)
Education and an awareness of ophthalmomyiasis amongst ophthalmologists working in rural areas are important for the timely diagnosis and treatment of this rather rare infestation. A thorough examination of the eye under magnification and prompt removal of the larvae could obviate the disastrous complications of internal ophthalmomyiasis. Public health measures such as the prevention of the exposure of farmers to the adult flies, and the killing of adult flies with insecticide sprays (e.g. malathion) will play a major role in preventing the disease and awareness of the disease will help to combat a disease which appears to be innocuous and yet is so serious – a disease that we believe is a silent endemic in certain rural parts of central India.
Footnotes
Acknowledgments
We are grateful to Dr K Ilango of the Zoological Survey of India, Hyderabad (Andhra Pradesh, India), who kindly identified the larvae.