
Abstract
SUMMARY
Internationally, teenagers are at risk for pregnancy-related morbidity and mortality. We assessed the obstetric and perinatal outcomes of teenage pregnancies compared with their older counterparts in northern Namibia.
We made a retrospective study using birth records from February 2002 to August 2002. The data collected included perinatal mortality, delivery mode, birth weight, in-hospital days and frequency of antenatal care (ANC) attendance. They were compared with primiparous women in different age groups (n = 612). No differences were found in obstetric and perinatal outcomes between the three different age groups. Overall ANC attendance was high.
The perinatal outcome for pregnant teenagers was comparable with their older counterparts in northern Namibia. In this region, ANC succeeds in reaching pregnant teenagers and teenage pregnancies are not at an increased risk for obstetric complications.
Introduction
Adolescents between 15–19 years give birth to approximately 13 million children annually. Over 90% of these births occur in low-income countries. 1 Without doubt becoming a mother at this very young age has major social implications. In most cases, the mothers are not married, they are not financially independent, their school dropout is high (either voluntarily or because they have been expelled) and the possibilities for further education while raising a child are limited. The medical consequences of childbirth at young age are unclear. The State of the World's Mothers 2004 state that pregnancy and childbirth are leading causes of death in teenage girls in low-income countries. This caused an influx of letters in the BMJ. 2
However, other studies of complications in teenage pregnancies present conflicting results on both maternal and neonatal outcomes. An increased incidence of maternal and perinatal mortality, preterm birth, cephalo-pelvic disproportion and low birth weight in teenage pregnancies has all been reported. 1,3–7 The variation in outcome of the different studies can be partly explained by differences in socioeconomic and cultural circumstances between regions and countries. 8,9
Cephalic pelvic disproportion (CPD), for example, has been described by some as an obstetrical complication in young teenage pregnancies. 3,5 Under favourable living conditions, growth in height ceases at 16–18 years of age, while pelvic growth ceases three years later. 3 However, in areas where living conditions are poor, the full development of maternal height and pelvis can be delayed and this could attribute to an increase of the incidence of CPD in older teenagers.
Another cause for obstetrical problems in teenagers in low-income countries is the increased vulnerability to pregnancy-induced hypertension, malaria and anaemia. This could explain a higher rate of intrauterine growth retardation and preterm birth. 3 In high-income countries teenage pregnancies occur mostly in lower socioeconomic classes 1 and an increase in obstetrical complications is mainly due to problems associated with nicotine, alcohol and drug abuse. 7 Adolescents are also at increased risk of abortion-related morbidity and mortality due to unsafe abortions. 10
In Namibia, approximately 15% of expectant mothers are under 20 years of age and 18% of teenagers have begun the childbearing process. 9 No local data are available concerning teenage pregnancy outcomes except for some early studies from South Africa where it was found that adolescence per se confers no increased risk for obstetrical complications. 11 However, black teenagers were at increased risk 12 as were unmarried motherhood among all age groups. 13
In this study, we assessed pregnancy outcomes of teenage primiparous women compared with their older counterparts in one of the two big hospitals in northern Namibia.
Materials and methods
Study site and population
The Onandjokwe district is situated in the Oshikoto region of northern Namibia and has one hospital, three health centres and 12 clinics. Onandjokwe Lutheran Hospital (OLH) is a 450-bed district and referral hospital serving a population of approximately 250,000, where comprehensive emergency obstetric care can be given. Primigravid women receiving antenatal care (ANC) in the region are advised to give birth at OLH and are allowed to stay in a maternity waiting home in the hospital compound from 36 weeks gestation onwards. During 2002, there were 3555 births of which 280 were by caesarean section (7.9%). There were three abortion-related deaths identified during a three year period, none of those patients were teenagers. 14
Data collection and analysis
We included all the primiparous women who gave birth to a singleton newborn in OLH from 13 February to 13 August 2002. Twins (n = 7) were excluded from the study. Data were collected retrospectively from the maternity records in the labour ward. Primiparous women were divided in three groups: 14–17 years (I), 18–19 years (II) and 20 years and older (III). The following parameters were compared between the three age groups: age, frequency of ANC attendance, trimester of first ANC attendance, mode of birth, birth weight, perinatal and maternal mortality, in-hospital days. Low birth weight was defined as less than 2500 g. When comparing low birth weight rates between groups, macerated stillbirths were excluded. In this hospital the definition of perinatal death includes all deaths occurring after 28 weeks gestation with weight greater or equal to 1000 g.
Data entry and analysis were done using Microsoft Excel, Windows 98. For statistical analysis, data were converted to SPSS version 14 (SPSS Inc., Chicago, IL, USA). For non-parametric data, P-value were calculated by the Mann-Whitney test, for binomial distributions χ2 test with Yates correction for 2 × 2 tables were used. Statistical significance was assumed if P < 0.05.
Results
During the six month study period there were 1735 singleton births in OLH. Of these, 605 (35%) were from primiparous women. The age distribution is shown in Figure 1 – the age was unknown in seven cases leaving 598 cases for analysis. The average age at birth in this group of primipara was 21.4 years (median 20, range 14–41 years). Only 5% of the primiparous women were over 30 years of age. There were no cases of maternal mortality recorded in the study group. The perinatal mortality rate for the total population of primiparous women was 26.4/1000 live births: eight were macerated stillbirth (1.3%), two were fresh stillbirth (0.3%) and six were early neonatal deaths (1.0%). For both fresh stillbirths, the age of the mother was unknown. No differences were found in the perinatal mortality between the age groups (group I versus group II, P > 0.1; group I versus group III, P > 0.5; group II versus group III, P > 0.1) (Table 1).
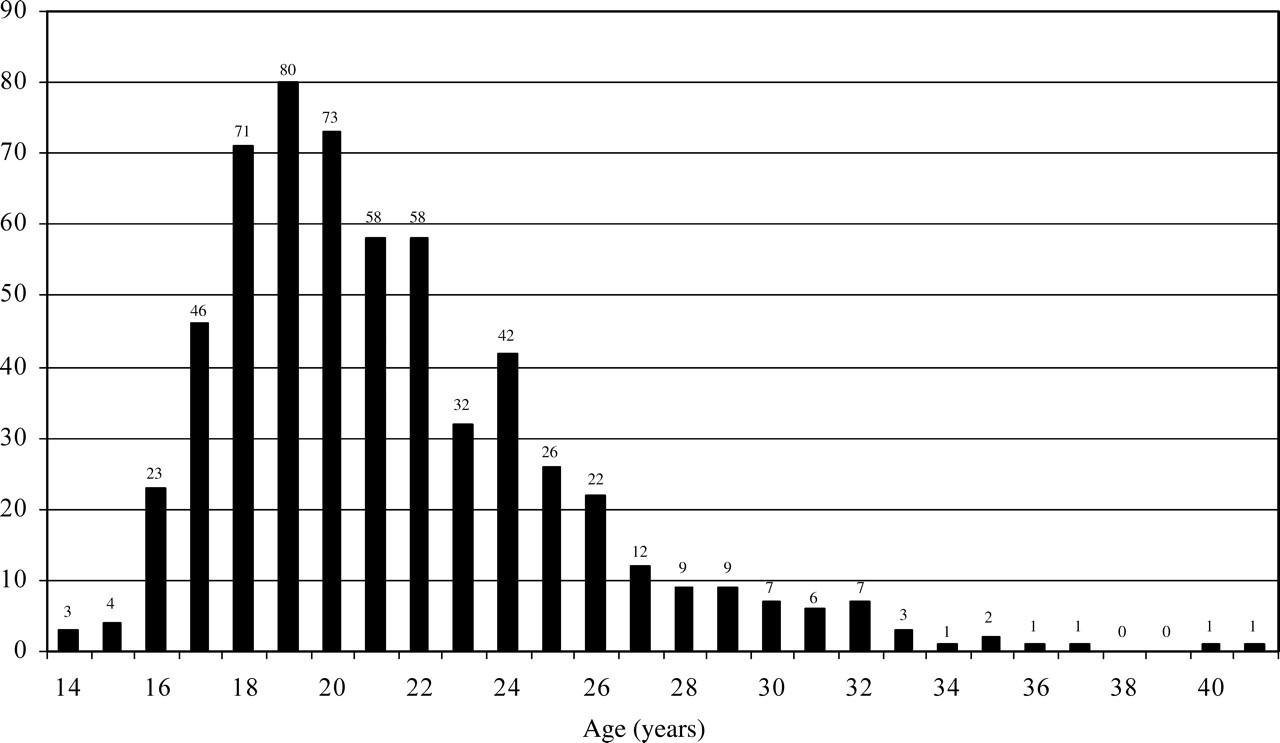
Age distribution of primiparous deliveries at Onandjokwe Lutheran Hospital, Namibia, from February – August 2002
In-hospital days (mean, 95% confidence interval, CI), caesarean sections (number + percentage) neonatal outcome and antenatal care (ANC) visits of primiparae according to age groups
aTotal caesarean sections 38, in one case age was unknown
bExcluded: macerated stillbirths
Of the 605 births, 567 were normal vaginal births and 38 babies were delivered by caesarean sections (6.3%). The mode of birth did not differ significantly between the age groups, although the caesarean section rate seemed to increase with age (group I versus group II, P > 0.5; group I versus group III, P > 0.1; group II versus group III, P > 0.1) (Table 1). There was no difference between the three age groups concerning average number of in-hospital days (group I versus group II, P = 0.64; group I versus group III, P = 0.87; group II versus group III, P = 0.60), ANC attendance or trimester of first ANC visit (Table 1). Overall, ANC attendance was over 93%.
The average birth weight was 2868 g (median 2900 g, range 950–4000 g). Birth weight did not differ among the study groups (group I versus group II, P = 0.94; group I versus group III, P = 0.83; group II versus group III, P = 0.74). The total number of low birth weight babies was 76 (13%). The percentage of low birth weight babies was highest in the very young teenagers (56% of women age 14–15 years, n = 7) and in the elderly primipara (100% in women >40 years, n = 2).
Discussion
Comparing perinatal outcomes in teenage primiparae with primiparae of the older age groups, we found no difference in maternal and perinatal deaths, birth weights, modes of birth or lengths of hospital stay. The small sample size and the short period of time during which the study was conducted may have affected the results of this study. Furthermore, a retrospective analysis of maternity ward records could cause one to question the trustworthiness of the data. As is often the case in rural African hospitals, however, no other information resources were available. An analysis of existing records can help to identify factors that are of local importance. In this case it seems to show that, unlike what was expected, teenage pregnancies in northern Namibia are not at risk for obstetric complications.
Overall ANC attendance was high (>90%), and ANC attendance among teenagers was no different from the attendance of the older nulliparae. Apparently, ANC in the Oshikoto region has succeeded in reaching women of all age groups. It seems that in this community pregnant teenagers are not socially disadvantaged. Two recent reports also found ANC to be an important factor in preventing poor obstetric outcome in teenagers. 15,16
The 2001 census reported 4034 births in the Oshikoto region of which 10.7% were to teenagers. The percentage of teenage primiparae delivering at OLH is 13%, indicating that the referral system, where high-risk pregnancies (like teenage primipara) are advised to deliver in the hospital, is working. Using the reported crude birth rate of 30.5, the regional annual births were expected to number approximately 4575. 9 Using both figures, it is calculated that between 75%–86% of births occurred in hospital, which is comparable with the national statistics. 9 The fact that 35% of all women delivering at the hospital are primiparae while the total fertility rate in Namibia is 4.7 also supports the idea of a working referral system for high-risk pregnancies. Probably most primiparae from the region deliver at OLH, while multiparae deliver at rural hospitals. Unfortunately, no data from these hospitals is available. Interestingly, the percentage of low birth weight births was higher in the older primiparae than in the younger. This is in contrast that which is usually reported. Unfortunately, in the maternity records no distinction was made between prematurity or low birth weight (i.e. small for gestational age). We recommend that the (estimated) term of delivery be included in the maternity records for future evaluations. Our results do not seem to show that teenage primiparous women have an increased risk for CPD in the Onandjokwe district. Although the low number of very young pregnant teenagers does not allow any strong conclusion, it is of interest that the percentage of caesarean sections in primiparae of 18 years and younger is low compared to older primiparous women. Furthermore, it is a positive sign that the number of very young pregnant teenagers (<16 years) is very low, which is also reflected in teenage pregnancies throughout Namibia. 9