
Abstract
A cheaper version of a self-illuminated proctoscope which suitable for use in developing countries designed for diagnosis and intervention in anorectal diseases is described.
Introduction
The proctoscope is still an invaluable anorectal pathology instrument but it requires a reliable source of illumination. This is a simple, cheap design of the age-old instrument.
Discussion
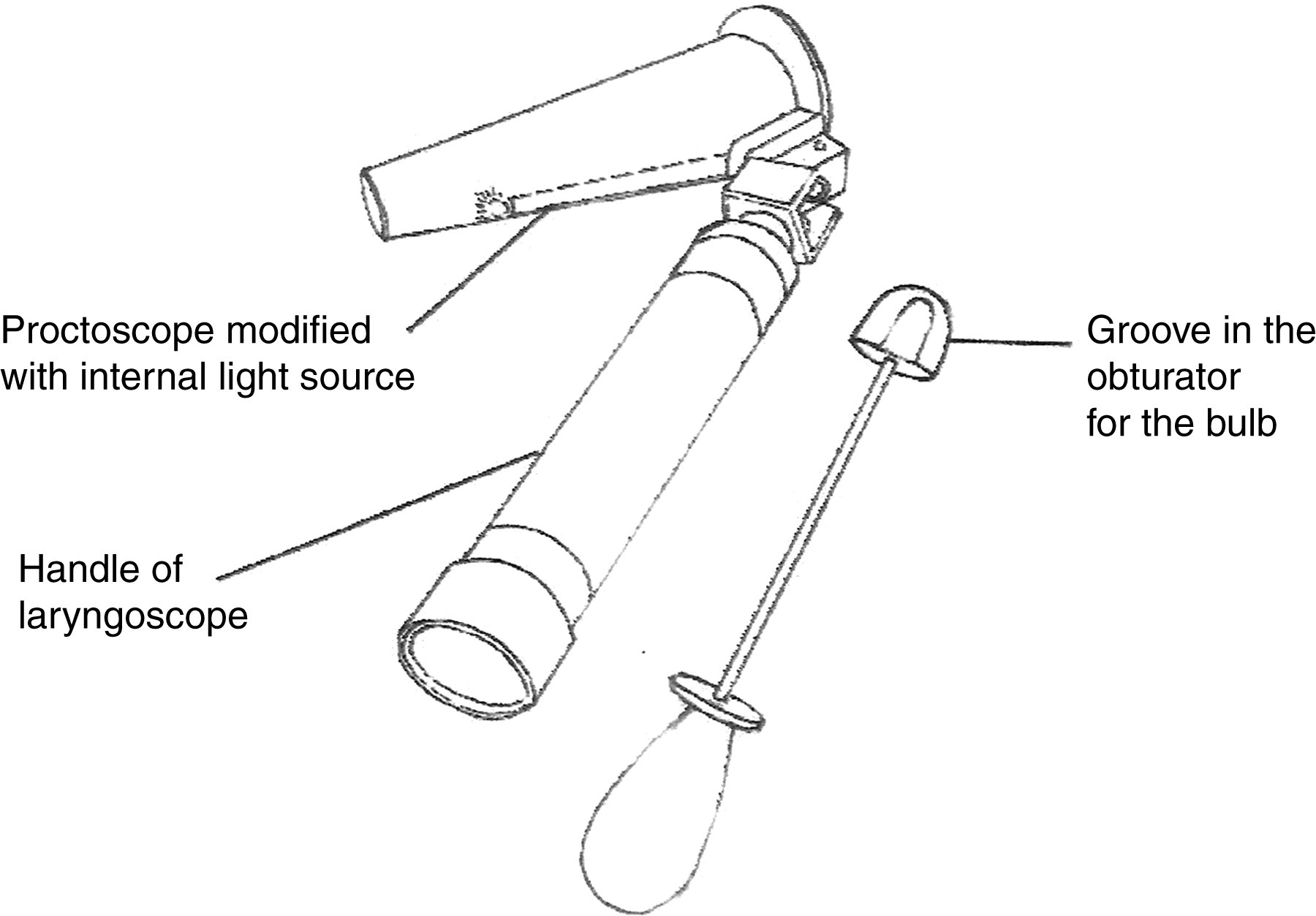
The instrument contains two parts: one is the handle of a standard laryngoscope containing batteries and the other is the speculum portion of the proctoscope (length 9.5 cm, tip diameter 2.2 cm and base diameter 4.7 cm) with a bulb and wire incorporated in a groove in its floor (Figure 1). The obturator has a vertical groove to enable it to slide smoothly over the bulb and the wire. Like the laryngoscope, the speculum can be detached, cleaned and disinfected. The concept was developed in the department of surgical gastroenterology in the Medical College, Calcutta. Subsequent trials and the final instruments were undertaken by R D Surgical Inc of Kolkata and it is already commercially available in Calcutta. The cost of the instrument is less than Rs 100 (US$2.5) and the bulbs cost only Rs 5–10 (US$ 0.13–0.25).
The self-illuminated proctoscope
Cylindrical tubes for rectal examination were used in the mid-19th century when lighting was reflected from external sources such as mirrors, kerosene lamps, candles and electricity. 1 Many different tubular proctoscopes are used today but they are all derived from the original Kelly type. They vary in length, calibre, shape of the tube (cylindrical/slightly conical), terminal openings (transverse/oblique), side slits, grooves, sliding attachments and methods of illumination. The most commonly used proctoscope is the St Mark variety (length 7 cm, diameter 2.2 cm at the tip and 3.2 cm the base) with a fibre-optic light source. 2–4 Disposable varieties are normally used nowadays. Fibre-optic light sources and disposable instruments are costly. The problem with the simple proctoscope is that the external light source for illumination seems inadequate in many situations, e.g. when injecting sclerosants, banding haemorrhoids or taking biopsy from small lesions. This design described above solves the problem in an affordable way.
Conclusion
This cost effective improvization of a very useful tool should be welcomed by developing countries with constrained health budgets.