
Abstract
Although the pathology of Crimean Congo haemorrhagic fever (CCHF) is mainly related to a haemorrhagic process with secondary cytokine storm, there have been no published reports of this fatal disease being a cause of diffuse alveolar haemorrhage (DAH). There are many aetiological factors emphasizing the direct role of endothelial injury on DAH. We present the case of a young adult Turkish man with diffuse bilateral alveolar haemorrhage without an episode of gross haemoptysis caused by the CCHF virus. Successful clinical results and a rapid clinical and radiological clearance were obtained within few days after starting daily oral ribavirin treatment. This fatal infection should be considered to exist in any patient presenting with DAH, and should rapidly be treated with ribavirin. Another very important factor which should always be borne in mind is the contagious character of the CCHF virus. It is one of the most dangerous microorganisms transmitted from person to person. Even the bronchoscopes contaminated with patient blood carry a high risk for nosocomial spread to medical staff and other patients.
Introduction
The syndrome of diffuse alveolar haemorrhage (DAH) denotes a diffuse intra-alveolar bleeding from small pulmonary vessels as a result of severe damage of the alveolo capillary membrane of the lungs. The clinical picture of DAH usually consists of haemoptysis, bilateral airspace opacification on the chest radiograph and a decreased haematocrit secondary to bleeding from the pulmonary microvasculature into the alveolar space. 1–3 Clinical and radiological features are not always distinctive from other causes of pulmonary findings. The clinical picture can vary from serious life-threatening acute respiratory failure to a more insidious presentation with minimal symptoms and without an abrupt haemoptysis.
Symptomatic cases of DAH are usually characterized by haemoptysis, respiratory failure and alveolar infiltrates on a chest radiograph. Haemoptysis may not be present in children and young adults as they may often have some difficulties with expectoration. If DAH is associated with an acute infection, such as leptospirosis or some other air-borne viral disease (etc. avian flu), the patient might not have the chronic respiratory findings seen in other chronic microvasculature pathologies. DAH is comparatively rare but can be a serious event.
The pathological mechanism of DAH is broad and has immunological as well as toxic, infectious, vascular, neoplastic and physical causes. It may also be a clinical manifestation of ongoing systemic diseases such as vasculitis syndromes or Wegener's granulomatosis. The rapid disappearance of radiological findings is more suggestive of alveolar haemorrhage.
Although there are many case reports and review articles describing causative mechanisms of alveolar haemorrhages associated with vasculitis and those from other factors, to the best of our knowledge, there has been no published no report of pulmonary haemorrhage in Crimean Congo haemorrhagic fever (CCHF).
Case history
A young adult male shepherd presented with a one-day history of nausea, diarrhoea, body aches, fever and skin rashes. He had reduced his oral intake and had occasional nose bleedings. He had no history of unconsciousness. On the admission, his temperature was 37.8°C and he had epistaxis and ecchymotic skin rashes on his forearms. Laboratory results showed extreme liver enzyme elevations. Peak levels were: alanine aminotransferase 748 IU/L (normal range 10–40); aspartate aminotransferase > 2500 IU/L (normal range 10–41); creatine kinase 510 IU/L (normal range 49–397) in the third day of admission; deep pancytopenia with platelets count of 1.1 × 1 p 3 /µL; and aPTT of 37 seconds (normal range 22–35 seconds) were noted without a deranged coagulation. The patient was referred from a CCHF endemic region from which, in previous years, the majority of Turkish cases had been observed, including the first index epidemic case seen in the year 2002.
The patient had a diagnosis of CCHF, according to the World Health Organization (WHO) case definition criteria on the initial day of his admission. 4 Immediately after being isolated in the clinic, he was given daily oral ribavirin according to the WHO recommendations. Laboratory results for polymerase chain reaction and immunoglobulin M specific serology (Refik Saydam Public Health Centre, Ankara, Turkey) confirmed the diagnosis after his recovery. He had a marked non-productive cough and crackles on both sides of his chest. The initial pulmonary artery chest radiograph demonstrated bilateral patchy alveolar infiltrates, which were interpreted as a possible bilateral/multilobar pneumonia or alveolar haemorrhage (Figure 1). Computerized tomography scanning of the chest two days later confirmed these findings (Figure 2). The patient's respiratory and haematological parameters improved dramatically without antibiotics and a chest X-ray taken on the fifth day of admission was normal (Figure 3). Thus, the diagnosis of alveolar haemorrhage was confirmed by greatly improved radiological findings.
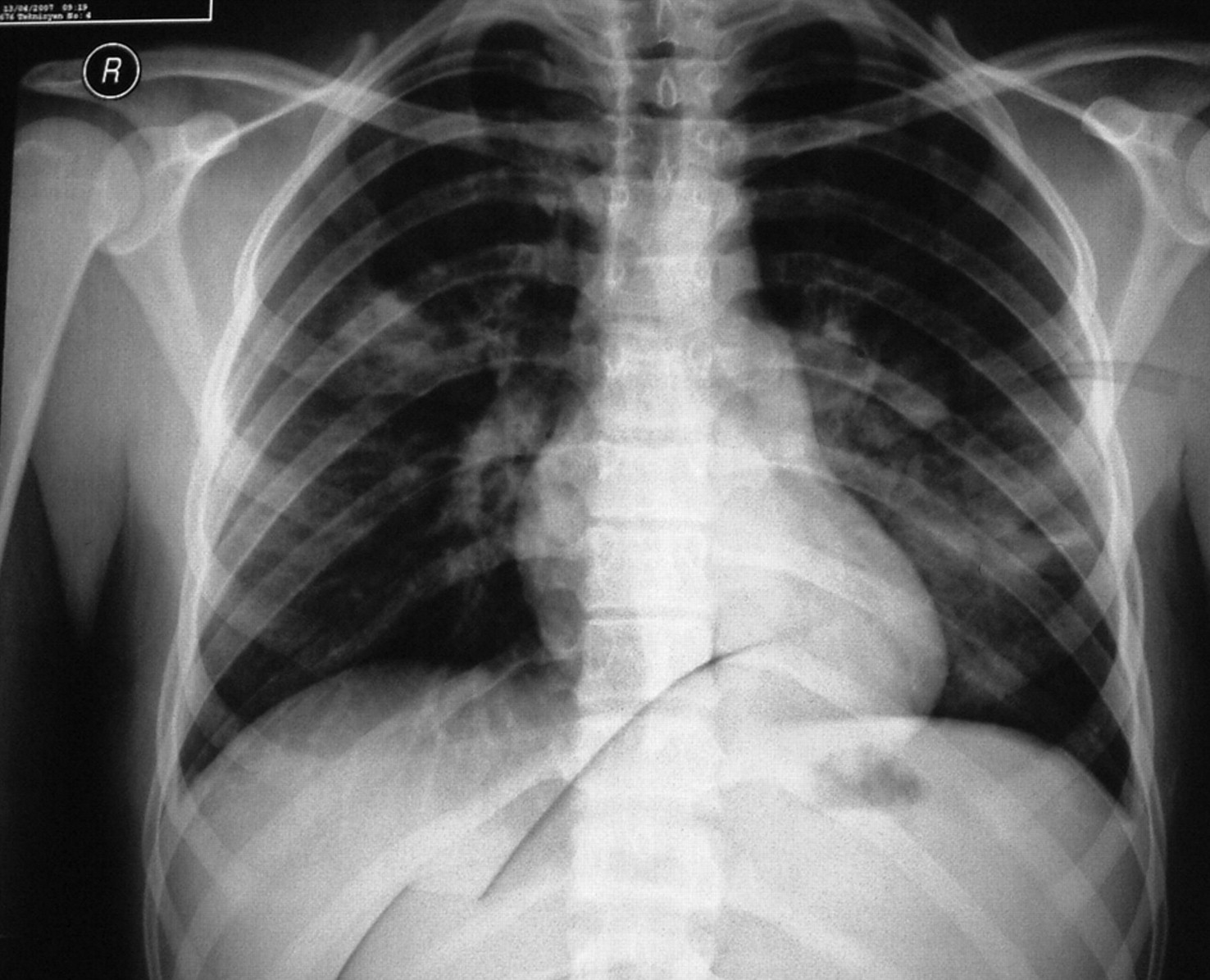
A chest X-ray showing bilateral patchy alveolar infiltrates

A computerized tomography scanning of the chest showing bilateral alveolar densities with ground-glass opacities due to airspace disease indicating an alveolar haemorrhage

A chest X-ray, taken five days after the first X-ray, demonstrated the resolution of the infiltrate
Discussion
CCHF, a viral systemic infection caused by a tick-borne virus occurs in the Middle East, Africa, Eastern Mediterranean countries and some parts of Eastern Europe. Humans are the only known targets for CCHF and health-care professionals are at great risk with secondary direct transmission and significantly increased fatality rates. The CCHF virus enters the human via a tick bite or a needle-stick injury to the skin or mucous membranes. Airborne infection is also a possibility. The disease appears after a short incubation period of two to seven days, spreading the virus to all parts of the body. 4,5 In severe cases of CCHF, illness begins abruptly with bleedings and high fever. Deep thrombocytopenia and other clotting abnormalities may occur. 6,7 The bleedings may range from some haemorrhagic skin rashes to profuse haematemesis and melaena; from vaginal bleedings to fatal central nerve system haemorrhages. During the clinical course of the disease, laboratory abnormalities include leukopenia, thrombocytopenia, elevated muscle and liver enzymes. A direct invasion of pulmonary interstitial tissue by the CCHF virus has not yet been reported. Our previous experience with daily oral ribavirin treatment has been successful when the drug has been used within first seven days, before the progression of macrophage-activating syndrome which is a terminal fatal mechanism of the immunological injury in susceptible patients. 7
In our case, the radiographic patterns showed diffuse snowflake-like densities corresponding to the areas of alveolar haemorrhage. Control radiographs showed good radiological progression from the alveolar pattern to all normal sequences. An overall progression in clinical and other laboratory parameters was seen within five days in the patient which suggests that ribavirin has a very effective therapeutic impact (Figure 4). Although deep thrombocytopenia and endothelial injury are the primary mechanisms of bleedings in patients with CCHF, it is not necessarily on the differential diagnosing list of DAH. 3,8,9 In the known epidemic regions, clinicians should keep in mind the possibility of the occurrence of this contagious infection, particularly since its nosocomial transmission has a significant fatality rate and contaminated bronchoscopes may easily transfer the infection in any clinical setting.
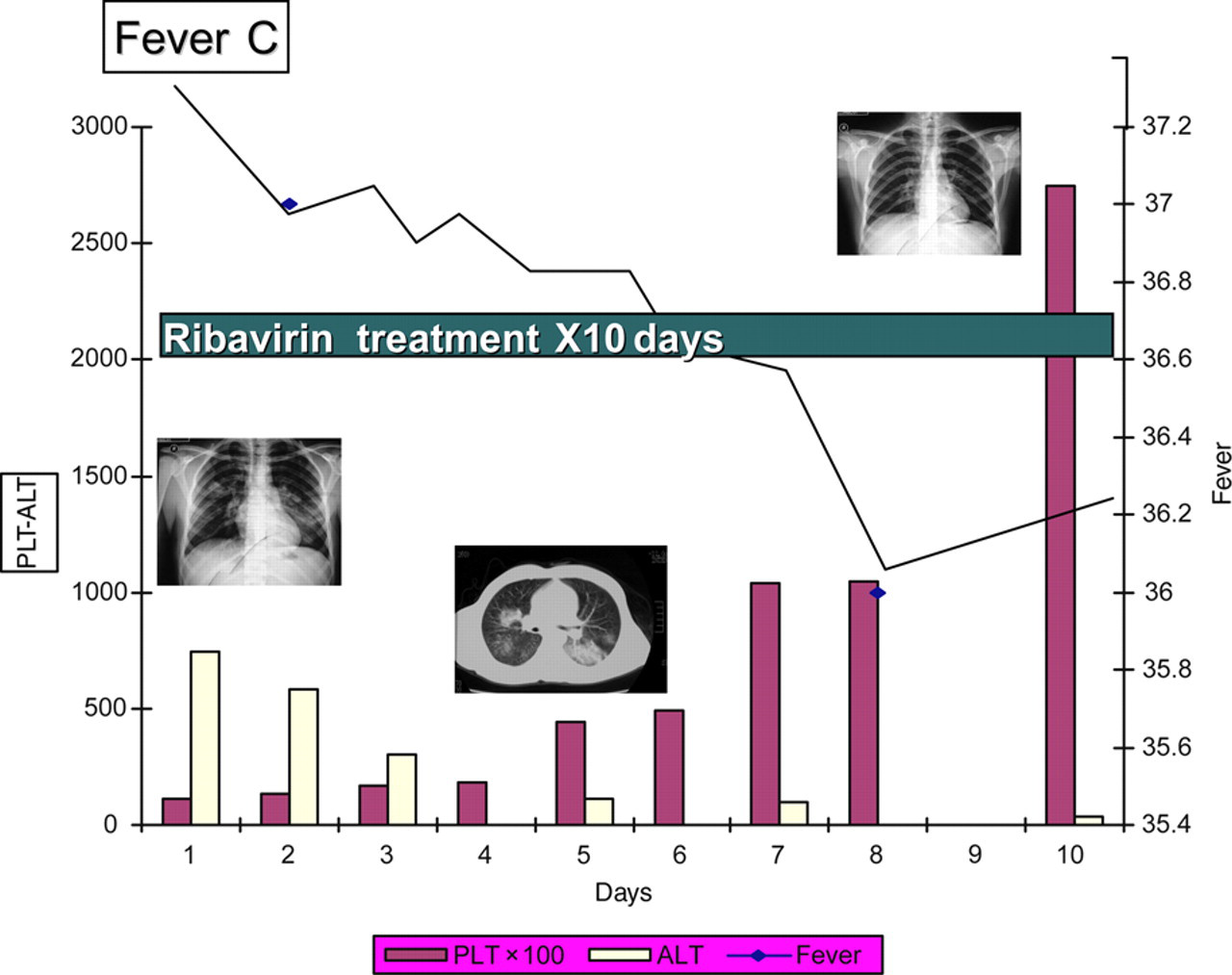
Clinical course of the infection
Footnotes
Acknowledgement
The authors are grateful Mrs Ayse Doganci for all her invaluable assistance in the preparation of the report.