
Abstract
Seven patients were treated for osteomyelitis rib (OR). Discharging sinuses and painful swellings were the presenting symptoms. An initial chest X-ray was unremarkable in all patients. Fine needle aspiration cytology and microscopy of pus did not reveal acid-fast bacillus in any patient. Computerized tomography (CT) of thorax was consistent with the diagnosis of OR in five patients. The patients underwent a subperiosteal excision of the affected part of the ribs or an excision biopsy of the unhealthy granulation tissue. Histopathological diagnosis was consistent with the diagnosis of tuberculosis (TB) OR in six patients. The patients received anti-TB drugs or appropriate antibiotics following surgery. All responded to treatment except one with a non-TB OR, who required further excision of the unhealthy rib ends. Inclusion of a CT of the thorax and an excision biopsy in the diagnostic process facilitates prompt diagnosis and effective management of OR.
Introduction
Osteomyelitis rib (OR) is a rare disease both in tropical as well as in temperate areas. 1 Due to its high prevalence, tuberculosis (TB) is an important aetiological factor for OR in India. The diagnosis is usually delayed by several weeks due to a lack of awareness and an absence of specific symptom and signs. 2 We present a report of seven cases and propose a strategy for prompt diagnosis and effective management.
Methods
The case records, chest X-ray, computerized tomography (CT) of the thorax, and cytopathology and histopathology slides of patients treated for OR at the Department of Surgery, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India, between December 2001 and August 2007, were reviewed. Additional sections from paraffin blocks were stained with a modified Ziehl-Neelsen stain to search for acid-fast bacilli (AFB). The patients were mailed follow-up request.
Results
Seven patients were treated for OR. The mean age of the patients was 23.7 ± 4.9 years (range 11–60 years). The male to female ratio was 1:2.5. The mean duration of symptoms was 38.9 ± 8.5 weeks (range 12–96 weeks). Two (29%) had earlier received anti-TB treatment on an empirical basis.
Four patients presented with a discharging sinus on the chest wall. Three presented with a painful swelling. Two of these were diagnosed as chest wall abscesses and were treated with incision and drainage. Microscopy of pus/fine needle aspiration cytology (FNAC) did not demonstrate AFB, and the chest X-ray was unremarkable in both the patients. They subsequently presented with discharging sinuses.
Cytopathology slides from three patients were available for review. The smears were poorly cellular comprising of a few inflammatory cells in the background of thin fluid. AFB was not demonstrated. A microbiological examination of the pus for AFB was negative in all three patients in whom it was undertaken.
An initial chest X-ray failed to detect OR in all of our patients, but repeat X-rays showed osteomyelitic changes in one patient who presented with a discharging sinus following an incision and drainage of a chest wall abscess. CTs of the thorax was undertaken in five patients which showed abnormal CT findings suggesting OR – i.e. the presence of soft tissue swelling, fluid collection, expansion of rib and/or lytic lesion in rib in the affected area of the chest wall (Figure 1).
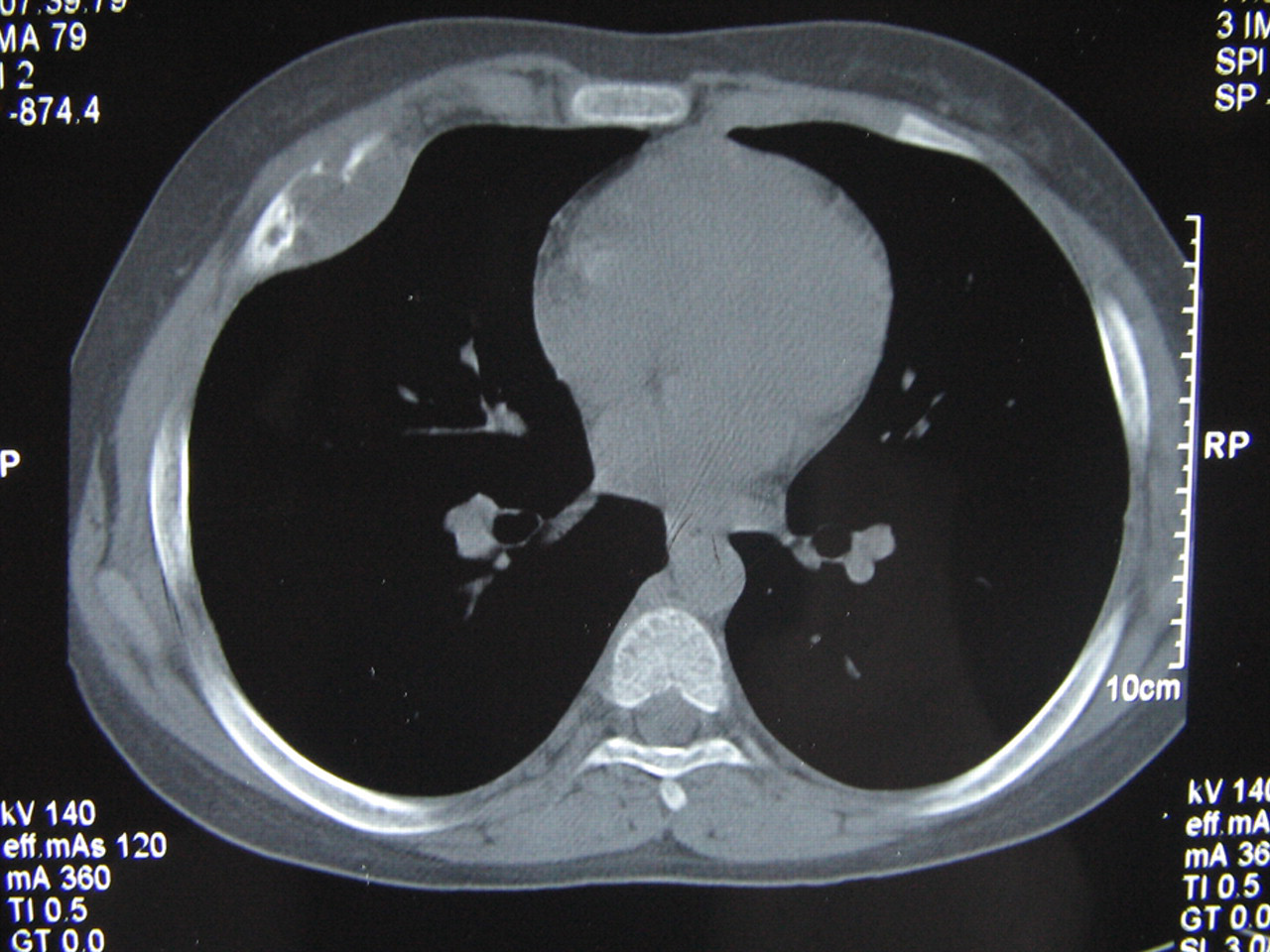
Computerized tomography of the thorax axial section bone window showing lytic lesions in the anterior end of a rib associated with an underlying convex fluid collection (attenuation value = 12 Hz)
Six patients underwent excision of a sinus and subperiosteal excision of an affected part of the ribs under general anaesthesia. In one patient, presenting with chest wall swelling, an excision biopsy of unhealthy granulation was done. The histopathology slides of seven patients were reviewed. Granulomatous osteomyelitis was seen in six. The tissue reaction patterns were epitheloid cell granulomas. Necrosis was seen in one case. AFB was not demonstrable in any of the patients. All these six patients received a full course of anti-TB treatment as per directly observed treatment short course (DOTS) chemotheraphy and recovered.
In one patient, the histopathology showed inflammatory granulation tissue with spicules of dead bone but no evidence of TB. The polymerase chain reaction was also negative for mycobacterium. The pus culture showed growth of Pseudomonas aeruginosa. The patient was treated with the appropriate antibiotics but required surgical re-exploration and further excision of unhealthy rib ends due to a persistent pus discharge. All the patients were well on follow up after periods ranging between four months to five years.
Discussion
A pus discharging sinus or a painful chest wall swelling are the two most common presentations of OR. Although OR is a clinically obvious diagnosis in cases presenting with a sinus, the differential diagnosis is much more extensive in case of a swelling on the chest wall because malignancies, such as Ewing sarcoma, fibro-sarcoma, multiple myeloma and secondaries from liver, breast, thyroid and kidney 3 are plausible diagnoses. However, aspiration of pus from the swelling or the detection of inflammatory exudates on FNAC indicates the possibility of OR. TB is considered the second most common cause of destructive rib lesions after metastatic neoplasm. 4
Routine chest X-rays sometimes failed to detect early skeletal disease and the diagnosis was often delayed until there was bone destruction with overlying soft tissue changes. 5 In comparison, a CT of thorax was useful for a complete investigation of rib lesions, characterizing soft tissue involvement, guiding biopsies and search for associated vertebral lesions. 6 Early radiological findings of OR include pericostal oedema demonstrated by soft tissue swelling of the thoracic wall accompanied by an adjacent inward pleural displacement. The bony changes appear one to two weeks later. The pericostal oedema can be readily diagnosed by an ultrasound scan. 7 An heterogeneous appearance and the presence of fluid filled cavities in soft tissue help to differentiate OR from tumours. 8 The CT of thorax suggested the diagnosis of OR in all the five patients.
FNAC was non-diagnostic in all three patients where it was attempted. Possible reasons could be non-representative sampling related to the inability to penetrate bone to obtain diagnostic material. The thin fluid aspirate resembled poorly cellular pus of the kind seen in a cold abscess, but the inability to demonstrate AFB resulted in the examination being non-diagnostic. Viewed from a different perspective, the FNA did exclude soft tissue extension of a neoplastic process in these patients, thus limiting the diagnostic considerations.
Microscopic examination – staining, culture or biopsy – is necessary in order to demonstrate TB bacilli for distinguishing tuberculous OR from non-specific OR, as well as for excluding other bone lesions, such as eosinophilic granuloma, congenital syphilis and malignancies which have similar radiological findings. 9 Granulomatous osteomyelitis was observed in six of the seven patients upon histopathological examination. The demonstration of AFB improves the diagnostic probability and a successful culture confirms Mycobacterium tuberculosis as the aetiological agent. Given the high endemicity of TB in our geographical context, it is not unusual to initiate treatment early in the diagnostic process and use a therapeutic response as a diagnostic tool.
We recommend a simple strategy for the management of patients presenting with a discharging sinus or a painful swelling on the chest wall (Box 1). Medical treatment alone is not sufficient, and a combination of wide debridement and an anti-TB drug regimen is essential in tubercular osteomyelitis of ribs. 10 In conclusion, the inclusion of a CT of the thorax and an excision biopsy in the diagnostic process facilitates prompt diagnosis and the effective management of OR.
A strategy for the prompt diagnosis and management of osteomyelitis of the ribs (OR)
Examine clinically to detect tender, thickened rib and/or associated intra-thoracic lesion Look for frank pus discharge, purulent aspirate or inflammatory exudates on FNAC to support diagnosis of an infective lesion Obtain CT of thorax early in order to diagnose OR Explore the lesion surgically and resect the diseased rib along with unhealthy granulation tissue Subject the resected specimen to histopathological and microbiological tests: Gram and Ziehl-Neelsen staining, pus culture for pyogenic organisms and mycobacterium and PCR if facilities are available Treat with appropriate antibiotics/ anti-TB drugs
FNAC, fine needle aspiration cytology; CT, computerized tomography; PCR, polymerase chain reaction; TB, tuberculosis