
Abstract
Pyomyositis is a subacute, deep suppurative bacterial infection of skeletal muscle not arising from contiguous infection. It is presumably haematogenous in origin, and characterized by muscle pain and swelling. We report on two patients who presented with pyomyositis in a tertiary care hospital in temperate region located in southern Brazil with a clinical presentation, which was initially suggestive of leptospirosis. This report discusses the pathogenesis, clinical presentation, diagnosis and management of pyomyositis. Physicians living in non-tropical areas should note that pyomyositis might occur in those areas, and its initial clinical presentation may be similar to leptospirosis
Introduction
Classically, pyomyositis is an infection of the tropics, occurring in previously active and healthy young men. 1 With increasing recognition from temperate regions, it is also referred to as non-tropical myositis, infectious myositis or spontaneous bacterial myositis. 2,3 Pyomyositis in temperate countries is often regarded as an infection that occurs in hosts who are immunocompromised or otherwise debilitated.
We report on two patients who presented with pyomyositis in a tertiary care hospital in a temperate region located in southern Brazil. Their clinical presentation was initially suggestive of leptospirosis. This report discusses the pathogenesis, clinical presentation, diagnosis and management of pyomyositis. Physicians living in non-tropical areas should be aware that pyomyositis might occur in such areas and its initial clinical presentation could be similar to leptospirosis.
Case history
Case 1
A 21-year-old white woman presented to the emergency room with a four-day history of flu-like symptoms, including generalized myalgias and fever. Examination of the extremities revealed very painful thighs, calves and the right arm, initially without oedema, fluctuation, erythema or warmth. Laboratory findings included a mild anaemia, leucocytes of 11,600 cells/mm3 (N 84%; L 11.5%; E 1.1%), aspartate aminotransferase (AST) of 56 IU/L, alanine aminotransferase of 78 IU/L. As there was the clinical possibility of leptospirosis, due to the epidemiology and clinical findings, empiric treatment with intravenous penicillin was started. A computerized tomography (CT) of the lower extremities showed several muscle fluid collections on the right and left thighs, and in the right and left calf muscles. Ultrasound-guided aspiration of the biggest thigh lesion revealed purulent material. A culture was positive for oxacillin-sensitive Staphylococcus aureus. Blood cultures were positive for oxacillin-sensitive S. aureus. Leptospira testing (microscopic agglutination test) and HIV antibodies were negative.
The patient improved clinically after antibiotic treatment with oxacillin and ultrasound-guided aspiration of the lesions.
Case 2
A 46-year-old white, previously healthy man presented with a five-day history of fever, myalgias, right back pain, dysuria and dark urine. The patient denied any recent trauma but revealed exposure to rats in his house. Physical examination revealed fever (38°C), mild jaundice, a pulse rate of 102 and blood pressure of 120/70 mmHg. Examination of the extremities revealed tenderness on palpation of the thighs, calves and the right infrascapular area. Laboratory findings included a leukocyte count of 8250 cells/mm3 with 28% bands, serum creatinine of 1.5 mg/dL, serum bilirubin of 4.3 mg/dL, AST of 235 IU/L of 141 IU/L, alkaline phosphatase of 399 IU/L and creatine phosphokinase of 4035 IU/L. Urinalysis revealed 3+ proteins, >100 leucocytes, >50 red blood count. Urine culture grew S. aureus (100,000 colonies/mL) and blood cultures were negative. The patient was started on penicillin for presumptive leptospirosis. Serologies for leptospira, hepatitis A virus and HIV were negative. On day 6, the patient continued to have daily low-grade fever and worsening of right back and thigh pain. On physical examination he presented right infrascapular tenderness and oedema and also thigh tenderness with oedema and induration on palpation. A CT scan showed several muscle fluid collections including the right posterior thoracic wall, gluteal region bilaterally, right anterior thigh and posterior thighs bilaterally. Aspiration of the thoracic collection revealed purulent material and a culture was positive for oxacillin-sensitive S. aureus. The patient improved clinically after antibiotic treatment with intravenous oxacillin and ultrasound-guided aspiration of the muscle abscesses.
Discussion
The pathogenesis of pyomyositis is not clearly understood. Diminished local resistance in the setting of transient bacteraemia is usually invoked. In a review by Gibson et al., 2 predisposing trauma, including strenuous exercise in healthy persons, occurred in 50% of cases in the USA and less than 30% of cases in the tropics. The permissive role of minor muscle damage is suggested by the numerous reports of pyomyositis after vigorous exercise and athletic activity in previously healthy individuals in temperate regions. 4 As observed in our two patients, pyomyositis is most commonly caused by S. aureus. 5 Group A streptococci are probably next in frequency. In addition, multifocal infection affecting more than one muscle group may be present in 10–20% cases. 6 Pyomyositis is often heralded by local, crampy muscle pain. Within a few days of onset, the affected muscles become oedematous and is often described a woody rubbery quality. 7
At this early point, suppuration of the muscle is not yet seen, but mild leukocytosis and low-grade fever may be present. Considering its rarity in non-tropical areas and vague and non-specific clinical presentation, it is unlikely to be considered during an initial diagnosis. 8 Despite the fact that our patients complained of severe muscle pain, neither had an initial history of vigorous exercise or predisposing trauma, in addition to the clinical signs of muscle inflammation, oedema, erythema and tenderness. Moreover, the clinical findings - fever, myalgias, mild elevation liver enzymes and creatine kinase serum levels - in both patients were highly suggestive of leptospirosis. It would, therefore, be expected that physicians in this area would begin treatment with penicillin. Although serology testing for leptospirosis was negative for both patients, the diagnosis of leptospirosis cannot be ruled out considering that delayed seroconversions are common, with up to 10% of patients failing to serocovert within 30 days of the clinical onset.
Imaging is the most useful method for diagnosing pyomyositis. Plain radiographs are not sensitive, but in a few cases may suggest muscle enlargement, loss of muscle definition, obliteration of deep fat planes, gas in soft tissues and reactive changes in adjacent bone. CT will often detect muscle swelling and well-delineated areas of fluid attenuation (Figure 1) that display rim enhancement with contrast. 9
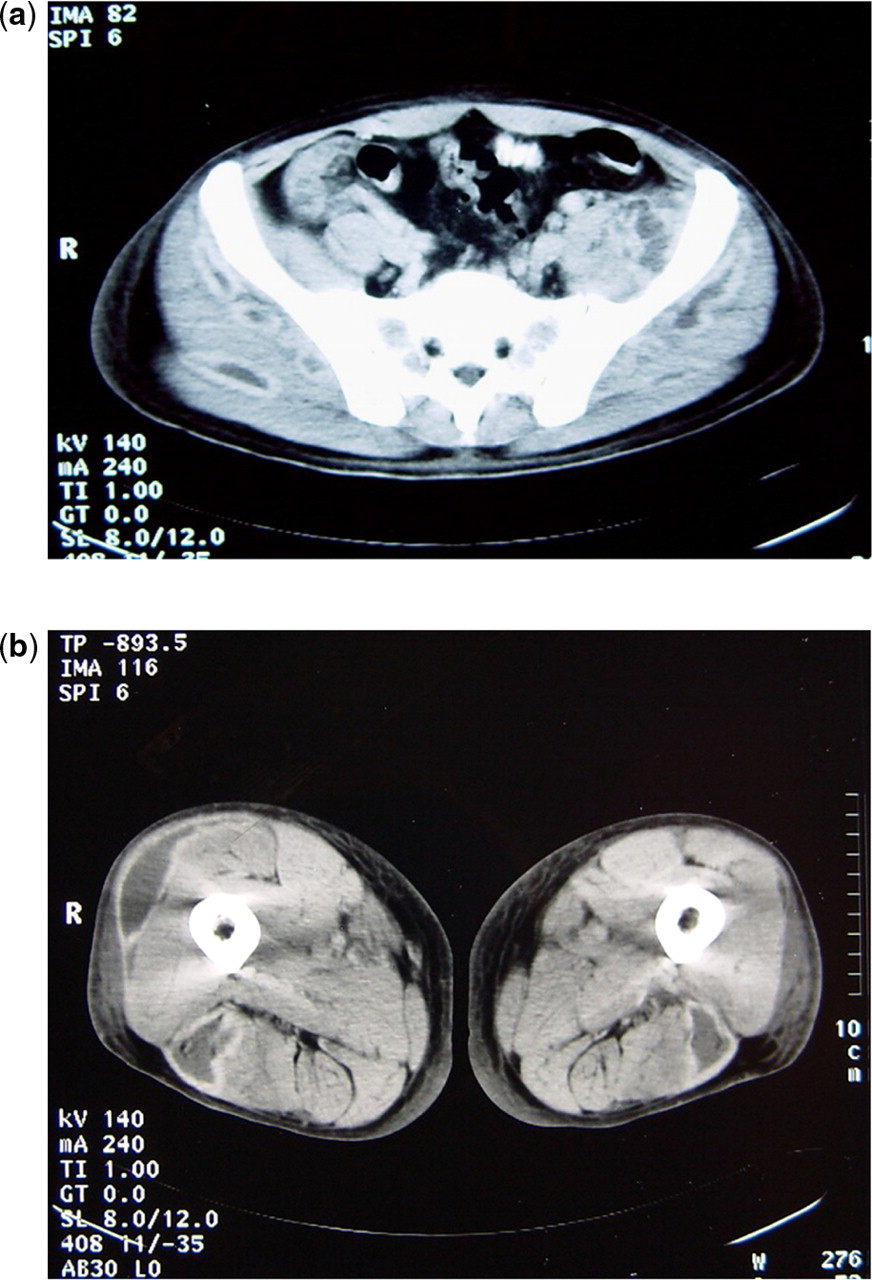
Computerized tomography scan of the lower extremities showing several muscle fluid collections on the right and left thighs (
Physicians living in non-tropical areas should be aware of the diagnosis of pyomyositis, which could sometimes be initially confused with other prevalent infectious diseases such as leptospirosis. Besides antimicrobial therapy, aspiration or surgical drainage of muscle abscesses are important therapeutic approaches for the eradication of the infection.