
Abstract
Primary amoebic meningoencephalitis (PAM) is not often seen. To date, less than 300 cases have been communicated to the medical literature since the disease was first discovered in 1965. Six of these reports originated in Venezuela. The authors describe a new spontaneous case of PAM in a 33-year-old previously healthy Western-Venezuelan man.
Introduction
During the first half of the twentieth century free-living amoebas were considered to be ubiquitous, non-pathologic protozoa. In 1958 Culbertson et al. 1 reported the pathogenicity of these organisms. In 1965 Fowler and Carter described the first case of amoebic meningoencephalitis (PAM) caused by Naegleria fowleri, a free-living, thermophilic amoeba that is found in soil and fresh water all around the world. It was previously thought to be an innocuous, harmless, saprophytic single-cell protozoan. 2 Since then, until 2006, just over 200 cases of the disease were reported in the medical literature. 3 The first PAM case that occurred in a Venezuelan national was described by Brass in 1972. 4 Since then a total of six cases have been reported. 3,5
We describe a spontaneous case of central nervous system (CNS) infection by N. fowleri in a 33-year old, previously healthy man from Western Venezuela.
Case history
A 33-year-old man presented with headache, fever, projectile vomiting, photophobia, nausea and disturbances of taste and smell 24 hours prior to his hospitalization. Upon admission the patient was lethargic. There was nuchal rigidity and a bilateral extensor plantar reflex. The Glasgow score was 9. The examination of the cerebro-spinal fluid (CSF) revealed numerous amoebic trophozoites which were grown in culture and identified as N. fowleri. His immediate family revealed that the patient had bathed in a fresh water swimming hole eight days previous to the onset of his disease.
During his second hospital day anisocoria was observed, and it was followed by fixed mydriasis. The electroencephalogram showed isoelectric activity. The patient was pronounced dead three days after the onset of his symptoms. Brain weight was 1.620 g. The meninges were hyperaemic and exhibited a discrete purulent exudate surrounding the congestive blood vessels. The orbito-frontal regions, olfactory bulbs and tracts displayed marked haemorrhage and necrosis (Figure 1). Microscopically, the leptomeninges showed an infiltrate consisting of abundant polymorphonuclear leukocytes and few lymphocytes. Numerous amoebic trophozoites were observed (Figure 2). The final neuropathological diagnosis was primary PAM caused by N. fowleri.

The basal aspect of the encephalon showing multiple foci of recent haemorrhage and necrosis and also purulent exudate surrounding the blood vessels
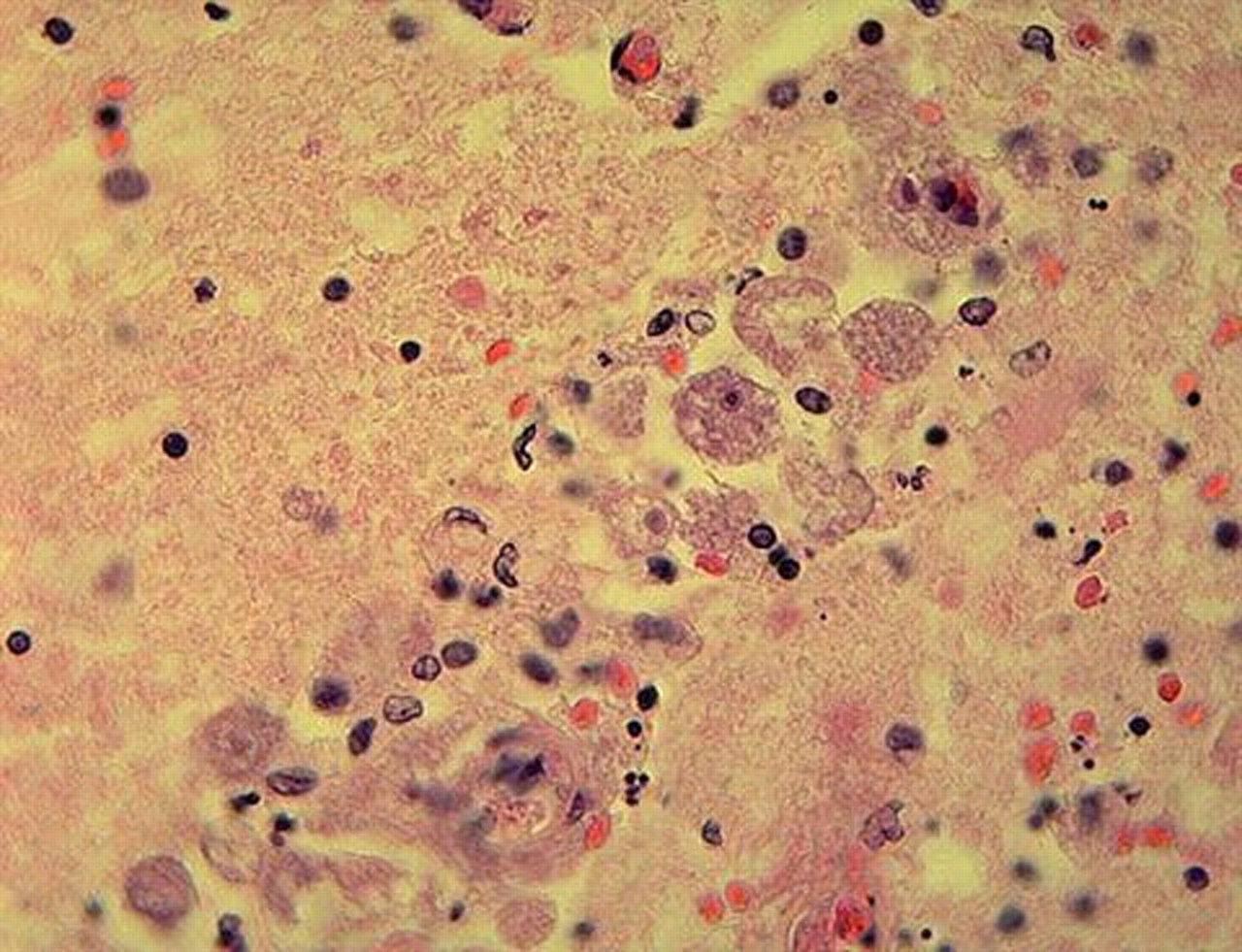
Naegleria fowleri trophozoites (H&E × 400)
Discussion
Free-living amoebas have the potential to cause three different neurological ailments in humans: PAM caused by N. fowleri, granulomatous amoebic encephalitis (GAE) and amoebic keratitis caused by protozoan organisms of the genera Acanthamoeba and Ballamuthia mandrillaris. 6 N. fowleri organisms are ubiquitous in nature and have a worldwide distribution. They are frequently found in fresh lakes, lagoons, swamps, pools and irrigation ditches. 6
PAM presents in generally healthy individuals who often have a history of swimming or playing games in fresh water reservoirs. 7 The neurological disease caused by these organisms consists of a fulminating clinical event that almost invariably leads to the demise of the patient soon after the onset of symptoms. A frequent diagnostic pitfall is to categorize these patients as harbouring bacterial meningitis, thus initiating incorrect clinical management.
The infection is originated by the contact of the nasal mucosa with water contaminated by trophozoites or flagellate forms of N. fowleri. The amoebae gain access to the olfactory bulbs through the ethmoidal cribiform plate and from there they colonize the meninges of the encephalon and the spinal cord as well as the underlying parenchyma, and cause a purulent meningoencephalitis. 6 Signs and symptoms appear two to five days after the exposure. The course of the illness is fulminant with a 95% mortality rate within five to seven days of its onset. 3,6
The symptoms are secondary to meningeal irritation, and they frequently include taste and olfactory disturbances, anorexia, headache, dizziness, confusion, and a rapid progression to coma and death. 8 From the neuropathological point of view, gross changes are characterized by a necrotic-haemorrhagic meningoencephalitis, with a modest purulent exudate that often is more evident in the lateral and basal aspects of the brain. Microscopically, trophozoites are observed around blood vessels. 3,6,8 These microorganisms resemble macrophages. Nevertheless, the conspicuous nucleolus evidenced by the protozoa allows differentiation. 3
The real incidence of cases of PAM and GAE is unknown because of an identification and reporting bias. Very often either viral or bacterial meningoencephalitides are held responsible for the neurological disturbances present in these patients. 3,6 In addition, the vast majority of the cases of CNS infection by free-living amoebas are diagnosed at autopsy, and the tendency in many countries is to keep the number of autopsies per year to a minimum. 3
The diagnosis of PAM should be considered in cases of meningoencephalitis with bacterial-free CSF. It is then mandatory to analyse the cerebrospinal fluid to detect free-living amoebas because the sooner the diagnosis is confirmed by the presence of motile unicellular organisms with pathognomonic broad, lobate pseudopodia, the sooner treatment can be started. 9